INTRODUCTION
This guide is designed to support cancer programs and care teams in delivering and coordinating care for patients with relapsed or refractory (R/R) follicular lymphoma (FL). Included below are insights from a national landscape analysis, including surveys, focus groups, and interviews with multidisciplinary providers, patients, and patient advocates. The guide explores 7 key domains related to care practices and highlights the experiences shared by those consulted throughout the project.
FL is a slow-growing type of B-cell non-Hodgkin lymphoma (NHL) representing approximately 20%- 25% of NHL cases in the US.1,2 While most patients initially respond well to treatment, FL typically follows a chronic, relapsing–remitting course in which periods of remission are repeatedly followed by relapse. With each subsequent line of therapy, response rates decline and diseasecontrol intervals shorten.2 Clinicians must navigate the disease’s clinical heterogeneity and weigh patient-specific factors such as age, comorbidities, and responses to previous treatments when selecting the most appropriate therapy.
The treatment landscape for R/R FL has evolved significantly in recent years with the introduction of advanced therapies, including cellular therapies and targeted agents. In the relapsed or refractory setting, second-line therapy often involves an anti-CD20 monoclonal antibody combined with chemotherapy, or lenalidomide with rituximab. Other anti-CD20–based regimens may be used in select circumstances. Although not preferred regimens, other second-line options include lenalidomide and anti-CD20 monoclonal antibody monotherapies.3

After at least 2 prior lines, advanced therapies—including chimeric antigen receptor (CAR) T-cell therapy and, more recently, bispecific antibodies (BsAbs)—are now important standards of care. Additional guideline-concordant later-line options include EZH2 inhibitors (especially for EZH2-mutated disease, with more limited benefit in wild-type), combinations of Bruton’s tyrosine kinase (BTK) inhibitors with anti-CD20 monoclonal antibodies, and investigational strategies combining anti-CD19 with anti-CD20 monoclonal antibodies.2-6 Given the rapidly evolving treatment landscape in R/R FL, this summary is not comprehensive. Patient care decisions should be informed by the most current evidence and published clinical guidelines.
TREATMENT CHALLENGES AND ACTIONABLE TIPS
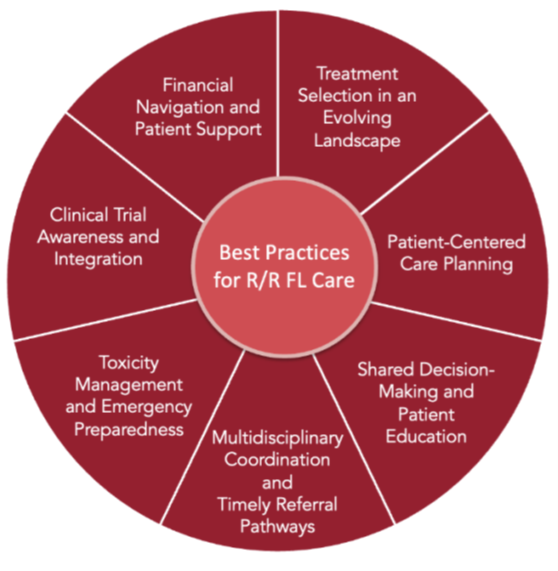
The sections that follow highlight effective care practices for patients with R/R FL. Each section explores treatment challenges and presents actionable tips across 7 key areas to support high-quality, coordinated care delivery.
Treatment Selection in an Evolving Landscape
With the growing number of available therapies, selecting the right treatment after relapse has become increasingly complex. Managing new options, including new therapeutic combinations, requires providers to stay current with emerging data and evolving standards. Providers noted that treatment sequencing is highly individualized and often depends on time to relapse, prior therapies, and patient-specific factors such as comorbidities and care goals. As novel agents move into earlier lines of therapy, the need for tailored treatment planning continues to grow.
Surveyed providers described a range of current sequencing approaches, including frequent use of combination regimens in earlier lines, such as pairing anti-CD20 monoclonal antibodies with chemotherapy or with lenalidomide. In the second-line setting, these regimens remain widely used, and novel CD19- and CD20-directed combinations are emerging as important options before moving to the third line. BsAb and CAR T-cell therapies were most often used in the third line and beyond, and combinations like BsAbs plus anti-CD20 monoclonal antibodies and lenalidomide are emerging in clinical trials at academic sites. These approaches illustrate the increasing complexity of treatment selection and sequencing in everyday practice.3
Providers also noted differences in how new therapies are reviewed and integrated across practice settings. At academic centers, clinicians may meet weekly to discuss individual patients, share new clinical data, and consider how emerging therapies or trials might apply based on individual treatment response and unique patient characteristics. Many community and rural practices report relying on external tumor boards or referring complex cases to specialists at larger centers for additional input and trial evaluation.
Practical Tips
Treatment After Relapse:
Additional Considerations for CAR T-Cell and BsAb Therapies:
Helpful Resources
Patient-Centered Care Planning
Care planning for patients with R/R FL requires ongoing flexibility to align with changing disease status, comorbidities, and individual care needs. Providers emphasized the importance of balancing efficacy, safety, and quality of life, particularly in later lines of treatment and in frail or older patients. They also recognized that addressing emotional, logistical, and financial needs is a core component of patient-centered care.
Patients and caregivers echoed these priorities, but some reported limited access to mental health services, financial counseling, and logistical support throughout their care. Certain practices can help close these gaps, such as screening for support needs, offering referrals to counseling services, and connecting patients and caregivers with peer support networks such as The Leukemia & Lymphoma Society (LLS), now Blood Cancer United, and the Lymphoma Research Foundation (LRF).
Practical Tips Patient Preferences:
Patient Psychosocial Needs:
Helpful Resources
Shared Decision-Making and Patient Education
Clear communication and shared decision-making are essential to R/R FL care. Yet, many patients report difficulty accessing reliable information and feeling fully empowered during treatment planning. Some patients describe diagnostic delays, limited explanations of available options, and the need to self-advocate for advanced therapies. Providers can play a key role by proactively supporting second opinions, explaining treatment choices clearly, and connecting patients to navigators or nurses who can help them access what they need.
Effective communication includes helping patients understand what to expect, responding to concerns in plain language, and creating opportunities for open and honest dialogue. Involving caregivers and drawing on educational tools, supportive services, and the broader care team can strengthen patient understanding and reduce overwhelm.
Practical Tips Shared Decision-Making:
Patient Awareness:
Supportive Environment:
Helpful Resources
Multidisciplinary Coordination and Timely Referral Pathways
Coordinated care is critical for patients with R/R FL, especially as they transition between community and tertiary care centers. However, managing complex, individualized therapies across diverse settings and care teams can be challenging. Some patients described confusion about care plans, delayed referrals, and difficulty navigating among providers and treatment sites.
Providers in the US Department of Veterans Affairs (VA) and rural programs noted additional coordination barriers, including limited access to clinical trials despite insurance coverage, lower health literacy, and difficulty arranging transportation to distant centers. To address these challenges, providers emphasized the importance of building strong referral relationships, using shared (or easily transferrable) documentation systems, and tailoring communication methods. Involving pharmacists in treatment planning and tumor board discussions can further support timely, safe, and well integrated care.
Practical Tips Academic Medical Centers:
Community Sites:
Pharmacist Role:
Helpful Resources
Toxicity Management and Emergency Preparedness
CAR T-cell therapy and BsAbs offer promising outcomes for patients with R/R FL, particularly in the third-line setting and beyond. These therapies require coordinated team readiness to manage severe, time-sensitive toxicities such as cytokine release syndrome (CRS) and neurotoxicity. Staffing levels, emergency protocols, training, and access to after-hours support may impact the ability to manage these risks, especially in settings with limited specialist availability. Beyond clinicians, pharmacists and infusion center teams play a key role in ensuring safe administration and appropriate follow-up care. Bolstering infrastructure, training, and communication across sites can help broaden access to these therapies while maintaining patient safety.
Practical Tips
Staff Training:
Adverse Event Management:
Pharmacist Support:
Helpful Resources
Clinical Trial Awareness and Integration
Clinical trials play a vital role in advancing care for patients with R/R FL. Some providers discuss trials early in the care process, while others wait until patients are more likely to be eligible, standard therapies have been exhausted, or trial options better align with clinical needs. Patient readiness is also a consideration, particularly at diagnosis, when individuals may feel overwhelmed. Even so, introducing the topic earlier can support informed decision-making and, in community settings, allow time for referral to academic centers when appropriate.
Clinical trial discussions and access can also be shaped by structural factors. Differences in staff capacity, clinical infrastructure, and patient support services across programs may affect how and when trials are introduced. Geography plays a significant role as well. Some providers refer to trials available within their own institutions, while others coordinate access through regional or academic partners, which may require patients to travel.
Practical Tips Access Barriers:
Community Sites:
Care Coordination:
Helpful Resources
Providers learn about trials from clinical trial finder tools, scientific meetings, peer communication, and research collaboratives.
Financial Navigation and Patient Support
Financial and logistical barriers can significantly limit access to advanced therapies for patients with R/R FL. Delays caused by insurance approvals, prior authorizations, and high costs are common, particularly in community and rural settings. Providers and patients noted that these challenges can delay treatment and add stress. Proactively addressing financial concerns and connecting patients with support resources can help improve access and reduce the burden of care.
Patients and providers reported success using hospital discount programs, charitable foundations, and clinical trial participation to offset financial burdens, particularly for nonmedical expenses such as transportation and lodging. Nurses, navigators, or care coordinators can discuss these resources in financial counseling sessions and consider developing a resource guide for patients on financial navigation.
Practical Tips
Insurance Considerations:
Financial Assistance:
Patient Support:
Helpful Resources
KEY TAKEAWAYS
Treatment for R/R FL is highly individualized and evolving, with providers balancing efficacy, safety, and patient quality of life while navigating complex sequencing decisions and emerging therapies like EZH2 and BTK inhibitors, CAR T-cell therapy, and BsAbs.
Multidisciplinary care coordination and timely referrals are critical to managing R/R FL, playing a key role in ensuring access to advanced treatments, clinical trials, and supportive care services, especially for patients in rural or community settings.
Persistent barriers—including insurance delays, limited access to clinical trials, and gaps in patient and caregiver support— highlight the need for greater emphasis on shared decision-making, proactive patient education, and structured care pathways.
References
1. Johnston K, Bennett M, Bains Chawla S, et al. Estimation of relapsed/ refractory follicular lymphoma patients on therapy in the United States. Blood. 2023;142(suppl 1):6148. doi:10.1182/blood-2023- 182030
2. Carbone A, Roulland S, Gloghini A, et al. Follicular lymphoma. Nature Reviews Disease Primers. 2019;5(1):83. doi:10.1038/s41572- 019-0132-x
3. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for B-Cell Lymphomas. V.2.2025. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed April 16, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org.
4. Casulo C, Barr PM. How I treat early-relapsing follicular lymphoma. Blood. 2019;133(14):1540-1547. doi:10.1182/blood-2018-08- 822148
5. Rivas-Delgado A, Magnano L, Moreno-Velázquez M, et al. Response duration and survival shorten after each relapse in patients with follicular lymphoma treated in the rituximab era. Br J Haematol. 2019;184(5):753-759. doi:10.1111/bjh.15708
6. Zinzani PL, Mayer J, Flowers CR, et al. ROSEWOOD: a phase II randomized study of zanubrutinib plus obinutuzumab versus obinutuzumab monotherapy in patients with relapsed or refractory follicular lymphoma. J Clin Oncol. 2023;41(33):5107-5117. doi:10.1200/JCO.23.00775
7. Binkley MS, Brady JL, Hajj C, et al. Salvage treatment and survival for relapsed follicular lymphoma following primary radiotherapy: a collaborative study on behalf of ILROG. Int J Radiat Oncol Biol Phys. 2019;104(3):522-529. doi:10.1016/j.ijrobp.2019.03.004
ACKNOWLEDGMENTS
ACCC wishes to thank the advisory committee who graciously gave their expertise and time to contribute to this resource.
Justin Arnall, PharmD, BCOP, FCCP
Clinical Pharmacist
Atrium Health Specialty Pharmacy Service
Charlotte, NC
Amy Goodrich, RN, MSN, BSN, CRNP-AC
Nurse Practitioner
Johns Hopkins Kimmel Cancer Center
Baltimore, MD
Aimee Hoch, MSW, LSW, OSW-C, FACCC
Financial Navigator
St. Luke’s Grand View Hospital
Sellersville, PA
Nakhle Saba, MD
Director of Lymphoma/CLL and CAR-T Therapy Program
Our Lady of the Lake Cancer Institute
Baton Rouge, LA
Danielle Shafer, DO
Medical Director for Malignant Hematology Clinical Research
Inova Schar Cancer Institute
Fairfax, VA
ACCC STAFF
Nicole A. Colwell, MD
Senior Editor/Medical Writer
Elana (Plotkin) Cerverizzo, CMP-HC
Senior Director, Education Programs
Kimberly Demirhan, MBA, BSN, RN
Assistant Director, Education Programs
Brittany Hansen
Director, Business Development
Michael Simpson
Marketing Manager, Education Programs
Carolyn Trachtenbroit
Program Manager, Education Programs