Author(s):
IN BRIEF
This study aimed to examine how patients with cancer navigated the challenges of oncology care during the COVID-19 pandemic, especially during the early phases of the pandemic. It specifically sought to explore the coping mechanisms of African American and White patients with cancer, detailing their personal narratives and the psychological, social, and emotional obstacles they faced. In this study, African American refers explicitly to individuals of African descent residing in the United States, acknowledging this group’s unique cultural, historical, and social experiences within the US. Study participants identified or used the terms Black and African American interchangeably as a personal preference in racial self-identification. Study results highlight the resilience of oncology patients, the critical role of support networks, and the efforts of health care providers to ensure continuity of care during this extraordinary global event.
In January 2020, the US diagnosed its first cases of COVID-19, marking the beginning of a public health crisis that would profoundly impact the nation. New daily cases peaked in mid-April,1 prompting widespread implementation of stay-at-home orders designed to minimize transmission. These measures were particularly crucial for vulnerable populations, such as older adults and individuals with compromised immune systems, who faced heightened risks of severe illness and mortality.2 Communities with higher exposure rates, predominantly those with lower socioeconomic status, limited access to health care, and racially diverse populations, were disproportionately affected, underscoring existing health inequities.3 These precautions disrupted daily life, strained health care systems, and exposed significant gaps in social and economic safety nets, further highlighting the pandemic’s far-reaching consequences beyond the immediate health risks.4
African Americans and Cancer
African Americans in the US experience significant disparities in chronic conditions and access to care, preventive screenings, and mental health support. They also have the highest incidence and mortality rates for several types of cancer compared to other ethnic groups.5 The American Cancer Society’s 2019 “Cancer Facts & Figures for African Americans” reports that both the incidence and mortality rates for all cancers combined are higher among non-Hispanic Blacks compared to non-Hispanic Whites, especially for prostate, lung, colorectal, kidney, liver, and pancreatic cancers.6 These disparities stem from a combination of biological and socioeconomic factors.
The publication, Health Coverage by Race and Ethnicity, 2010–2022, highlights that despite improvements from the Affordable Care Act (ACA), Black Americans remain uninsured at higher rates than White Americans. Factors such as lower access to employer-sponsored insurance, income inequality, and state-level Medicaid expansion disparities contribute to these ongoing inequities. For example, in 2018, the uninsured rate for Black individuals was 11.5%, compared to 7.5% for White individuals, and Black populations were more reliant on Medicaid coverage due to these systemic challenges.7
African Americans and COVID-19
The COVID-19 pandemic disproportionately affected African Americans and other communities of color.8 Approximately 97.9 out of every 100,000 African Americans succumbed to COVID-19, a mortality rate much higher than that of Latinos (64.7 per 100,000), Whites (46.6 per 100,000), and Asians (40.4 per 100,000). This exacerbated existing racial, socioeconomic, and health care access disparities, further perpetuating inequality. By mid-August 2020, the US had lost approximately 171,000 lives to COVID-19, with the heaviest impact on Black and Indigenous communities.9 Throughout the pandemic, communities of color continued to bear a disproportionate burden of disease. For instance, African American individuals experienced COVID-19 mortality rates similar to those of White individuals who were 10 years older.10 Another significant factor contributing to higher mortality rates among African Americans was their increased likelihood of working in essential jobs, such as health care, transportation, food service, and retail.11 As Dr. Anthony Fauci noted, many in the African American community held jobs that did not allow for remote work, making them more vulnerable to COVID-19.12 Additionally, crowded living conditions in urban areas increased virus transmission rates among racial and ethnic minorities.13 Research published in JAMA Oncology found that cancer patients diagnosed within the past year faced higher COVID-19 hospitalization rates (47.5%) and mortality (14.9%) compared to noncancer patients.14
This trend was exceptionally high among African American patients with cancer, for whom the dual burden of cancer and COVID-19 compounded health challenges. This patient population faced higher risks of severe outcomes due to immunosuppression from cancer treatments, as well as delays in care caused by pandemic-related disruptions in health care settings. These impacts dispropor-tionately affected African American patients with cancer, who
were already navigating barriers to equitable cancer care before the pandemic.15,16
Given the disproportionate impact of the pandemic, understanding how African American patients with cancer navigated these challenges became crucial to me as an essential worker and as an oncology social worker of color. The rapidly evolving nature of the crisis emphasized the need to document these experiences, not only for future research but as a means for me to process the
profound losses faced by my patients and myself. The political climate also further motivated this effort, as patients of both Black and White backgrounds, regardless of political differences, shared common feelings of fear, grief, and uncertainty during this unprecedented period. The political climate at the time was very divisive and continued to influence experiences within the health care setting. The few African American coworkers, including myself, were inundated with the haunting faces and cries of Breonna Taylor and George Floyd. Fears surrounding our mortality arose from COVID-19, the fears of police brutality, and the safety of people who looked like us. Black Lives Matter evoked pride but also took the mask off those who pretended to be allies or stood firmly against acknowledging the injustice and collective action of those we considered allies. The fears and concerns expressed by patients appeared universal, with shared emotions bridging racial divides. The initial anger and frustration and the need to tell the stories of African American patients evolved into curiosity. It sparked a more profound interest in exploring and documenting the experiences of both African American and White patients with cancer to understand the human connection and learn more about their coping strategies during this extraordinary period.
Methods: Participants and Procedures
This study was conducted in the Northeast from September 2020 to June 2021 and began after securing Institutional Review Board (IRB) approval. Eligible participants were identified by the oncology social worker based on their diagnosis and interest in the study. Participants had to meet the following inclusion criteria: (1) be 18 years or older, (2) be able to speak English, (3) have a diagnosis of metastatic solid tumor or hematologic cancer, and (4) be receiving treatment at The Cancer Institute at St. Francis Hospital in East Hills, New York. The oncology social worker introduced the study during participants’ treatment sessions, providing details and a pamphlet. Those interested signed a consent form. To ensure confidentiality, participants were anonymized for data analysis. A qualitative research approach was used, incorporating both in-person interviews, conducted with safety precautions, and phone interviews. Participants also completed the Well-Being Assessment Tool, a validated measure developed in the 100 Million Healthier Lives initiative led by the Institute for Healthcare Improvement. This tool evaluates health, well-being, and equity across multiple dimensions, including physical health, emotional resilience, social connections, financial security, and access to community resources.17 The tool addresses these interconnected areas and comprehensively views individual, organizational, and community well-being.
Measures: Informed Consents
In this study, informed consent practices began with a thorough explanation of the study’s purpose, providing participants with a clear understanding of the research objectives and potential contributions to future narratives about the pandemic. To ensure confidentiality and anonymity, participants were informed of the protocols to protect their identities throughout the data analysis and reporting phases. Permission was then requested to record each interview, including FaceTime and voice recordings, to facilitate accurate data evaluation. After obtaining consent, the researcher asked the interview questions, ensuring that participants felt comfortable and informed. Each session concluded with the researcher expressing sincere gratitude for the participants’ time and insights. Participants were reassured that the recordings would be securely handled and stored to maintain their privacy upon study completion.
Measures: Data Collection
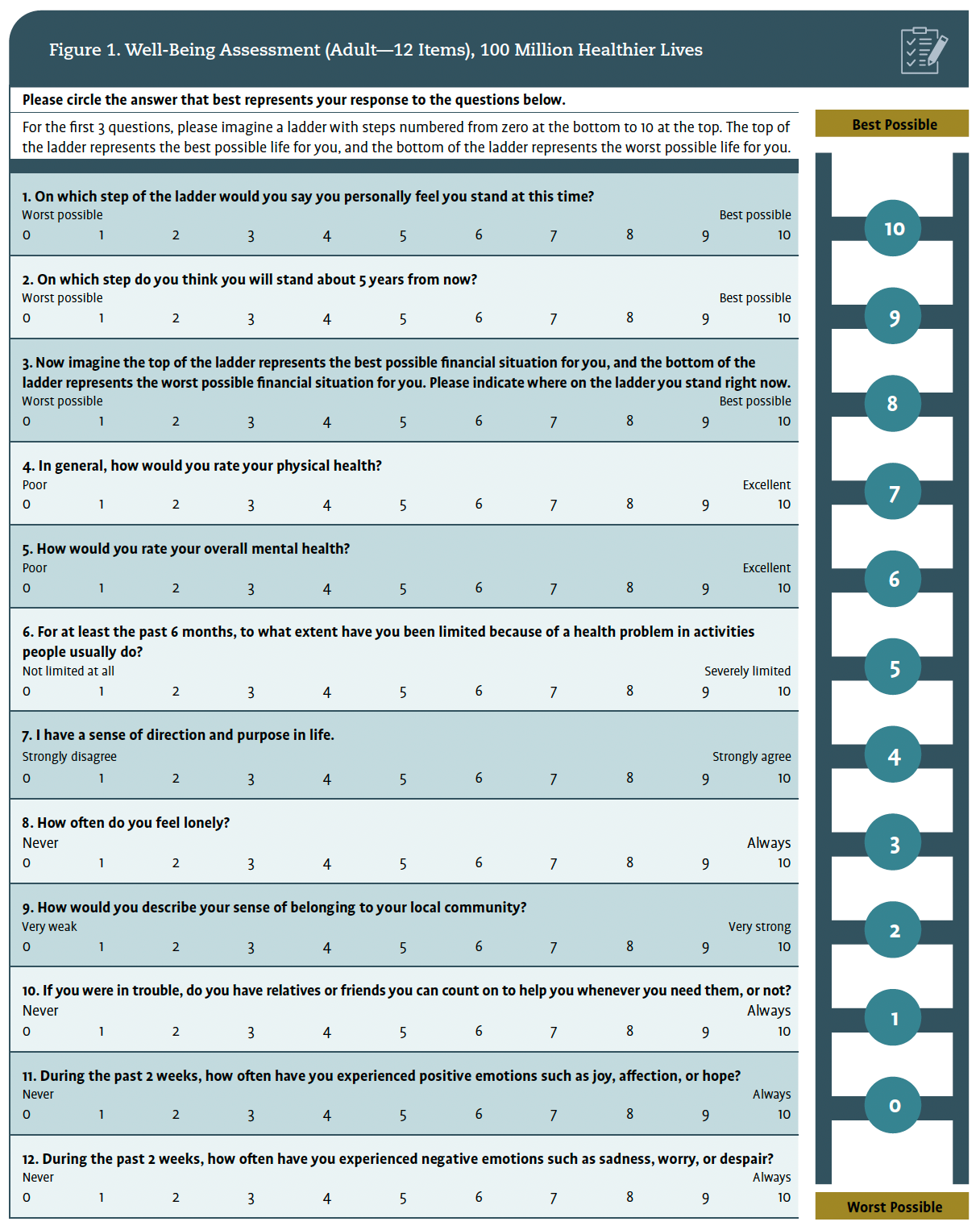
All interviews were recorded with the permission of each study participant. The oncology social worker took detailed notes during the interview. The oncology patients were asked for basic demographic data, including age, gender, race, marital status, education level, and county of residence. They were then screened using the Well-Being Assessment Tool for Adults developed by The Institute for Healthcare Improvement.17 This 12-item questionnaire, depicted in Figure 1, was administered to assess their physical and mental health.
The Well-Being Assessment Tool is a well-established, validated tool developed “as part of the 100 Million Healthier Lives initiative…[to] help individuals, organizations, and communities measure what matters most to advance health, well-being, and equity at multiple levels and across topics.”18 Each item of the survey questions was validated separately. Subsequently, the entire tool was validated through a comprehensive project involving a diverse, multicity sample of the US population.19
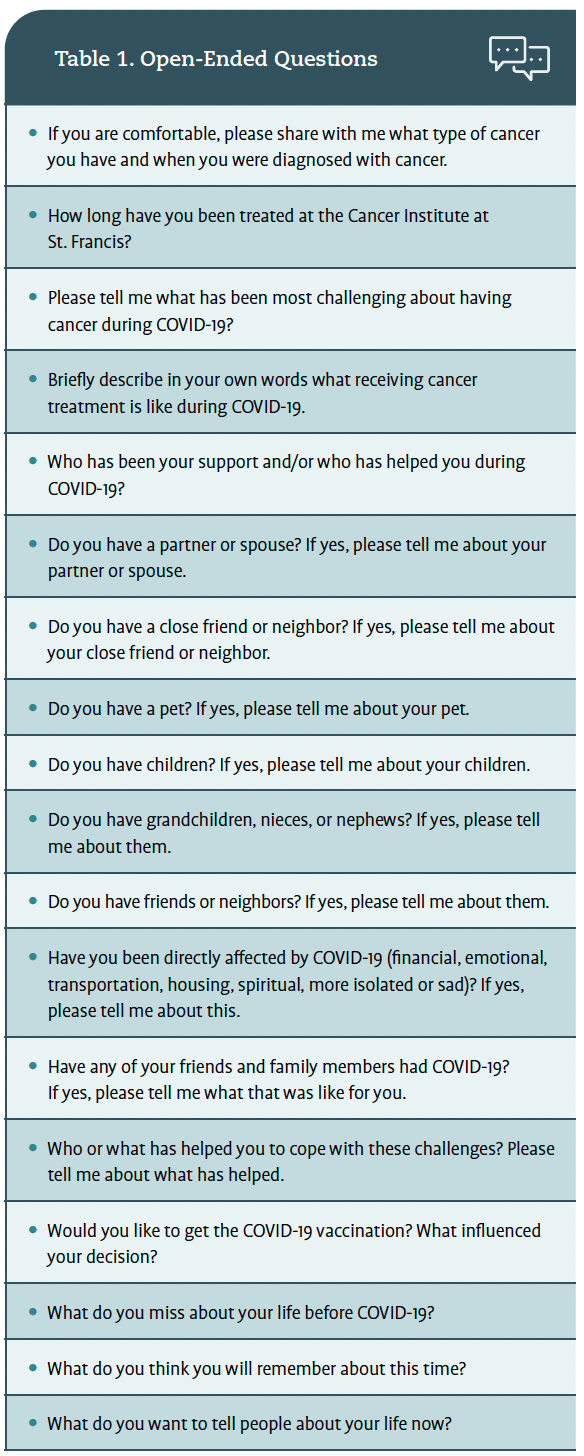
After completing the Well-being Assessment Tool, patients were asked open-ended questions regarding their diagnosis, cancer treatment regimen, relationship with their health care team, experiences during the COVID-19 pandemic, coping with social isolation, and their hopes for a post-COVID-19 world. Open-ended questions are key in qualitative research, especially exploratory studies. These questions allow participants to express their thoughts and feelings in their own words, offering researchers a deeper understanding of complex phenomena.20
Additionally, this method is particularly useful when engaging individuals who may be reluctant to complete surveys, as it provides them with the opportunity to articulate their perspectives more freely.21 This approach is especially valuable for reaching marginalized or hard-to-access populations, such as refugees22,23 or ethnic and religious minorities.24 Open-ended questions allow participants to provide a broader range of responses, resulting in richer and more diverse data than closed or forced-choice survey methods typically yield.21 This finding aligns with Padgett’s emphasis on the qualitative approach’s capacity to capture complex, nuanced perspectives, making it especially suitable for exploring sensitive or multifaceted social issues.25 By prioritizing depth over breadth, qualitative methods facilitate a more comprehensive understanding of participants’ experiences and contexts, enabling researchers to uncover meanings that may be inaccessible through quantitative methods.25 The open-ended questions from this study are shown in Table 1.
Data Analysis
Following the interviews, audio recordings were transcribed using Otter.ai, an automated transcription tool.21 Notes taken during the interviews and insights from postsession debriefs were also incorporated into the analysis to deepen the understanding of participants’ experiences. Field notes and post-session debriefing notes were used to enrich interpretations. Statistical analysis and quantitative data collection were performed using standard spreadsheet tools in Microsoft Excel software.

Quantitative Results
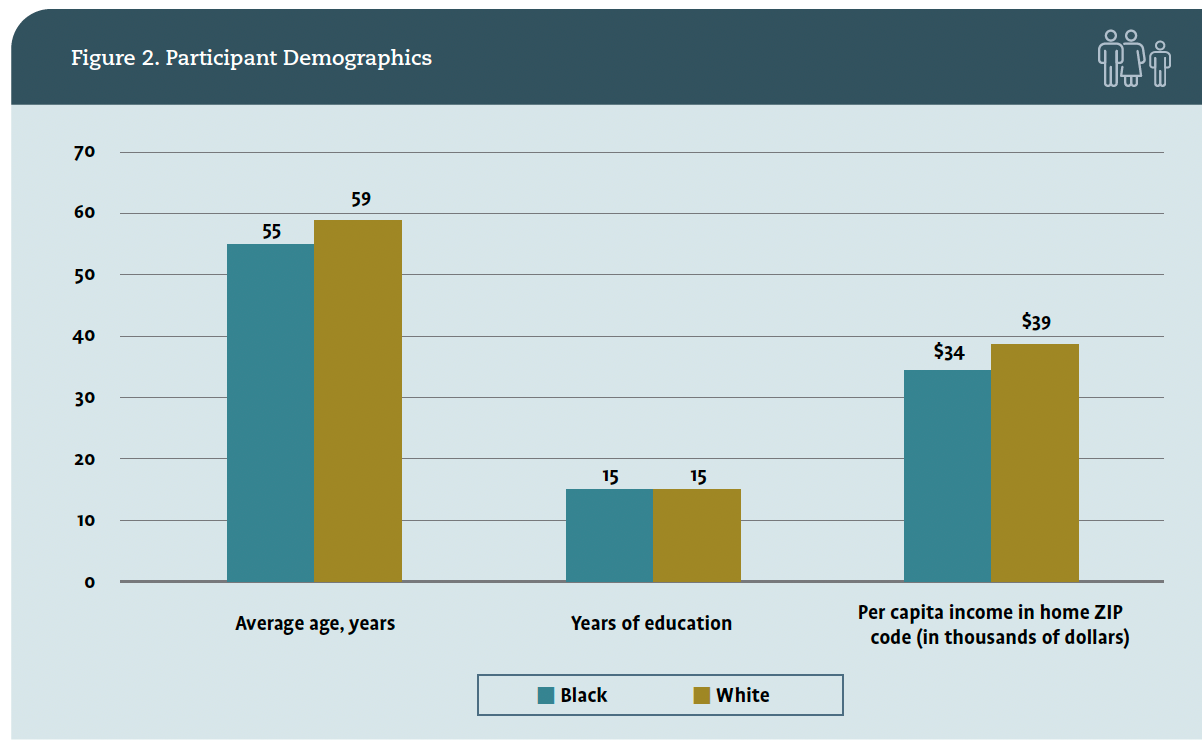
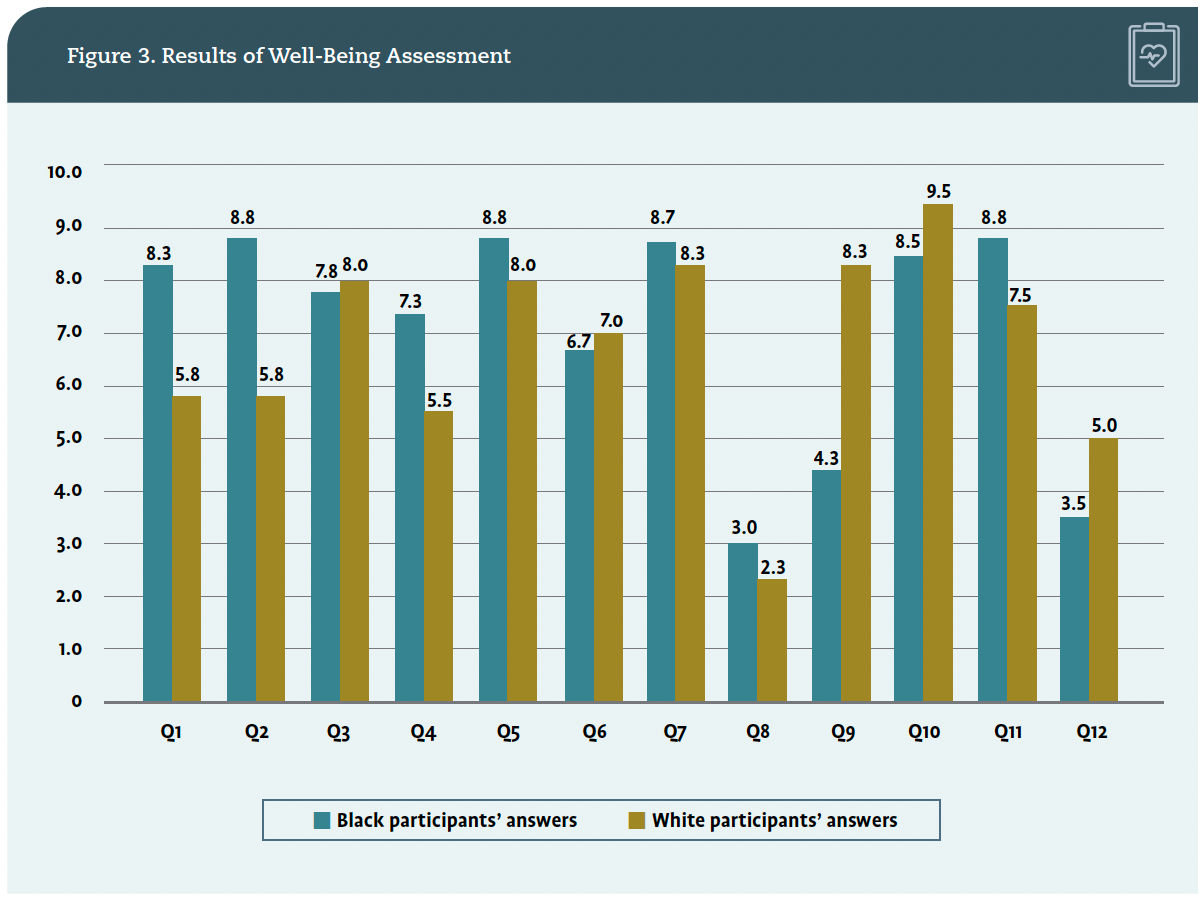
The study consisted of 4 African American and 4 White patients. Participants’ ages ranged from 45 to 68, with a median age of 55. The sample included 5 women (63%) and 3 men (37%), specifically 3 African American women, 1 African American man, 3 White men, and 1 White woman, ensuring a mix of gender and racial representation. Education level, determined by the Well-being Assessment Tool, was converted into years for comparison, and ZIP codes were used to assess the average per capita income of the participants’ home areas.17 Half the participants were unmarried (n = 4; 50%). No significant differences in age, years of education, or per capita income between White and African American participants were found. Participant demographics are listed in Figure 2. Well-being assessment questions were compiled, averaged, and compared across groups of participants, as presented in Figure 3.
Most of the well-being questionnaire answers provided by the subjects did not vary significantly between the races. There were, however, some notable differences between African American and White study participants. For the question, “On which step of the ladder would you say you personally feel you stand at this time?” the average step chosen by African American participants was 8.3, while the value was 5.3 for White participants. Similarly, Black study participants felt that 5 years from now, they would be doing better than White subjects thought they would be doing (8.8 vs 5.8). Another question with dramatic differences in responses was asking, “How would you describe your sense of belonging to your local community?” Black patients averaged 4.3 on a 10-point scale, while White patients’ average value was 8.3.
Qualitative data analysis revealed 5 emergent themes across both racial groups: the support and value of the oncology care team, the importance of social and family support, familiarity with safety precautions and isolation that predated COVID-19, the stress of isolation during COVID-19, and future planning.
Qualitative Results
Theme 1. Support of the Oncology Team
African American and White participants emphasized the significance of continuing treatment during the pandemic. Five of the 8 participants cited the relief of receiving care despite the risks of COVID-19, with safety protocols in place making them feel secure. One participant noted that receiving treatment helped them to maintain a sense of connection in an increasingly isolated world. Others appreciated the consistency of the chemotherapy routine, especially in the absence of family support. For example, 1 participant reflected on the positive atmosphere at the treatment center, stating, “Everyone is so nice and tries to keep your mind off things, focusing on other matters instead.”

Theme 2. Importance of Family and Social Support
Participants from both groups described the essential role family, friends, and neighbors played in reducing the anxiety and fear triggered by the pandemic. The uncertainty surrounding COVID-19 heightened feelings of helplessness and isolation, alleviated through support from close networks. Statements like “My pastor always called to ask what I needed” and “My neighbors checked on me every day and helped with groceries” highlight the importance of community during this time.
Theme 3. Familiarity with Safety Precautions and Isolation Preceding COVID-19
Many participants, particularly those with blood cancers or who had undergone stem cell transplants, noted that they were already accustomed to precautions like wearing masks and social distancing before the pandemic. For these individuals, COVID-19 safety mandates did not drastically change their behaviors. One participant noted, “I was already acclimated to those conditions.” Both Black and White patients with cancer experienced a shared sense of isolation and increased caution around family and friends due to concerns about contracting COVID-19. Many of these individuals shared that they were already immunocompromised and were accustomed to taking extra precautions to protect themselves from illness. They continued to practice these behaviors during the pandemic.
Theme 4. Stress of Isolation During COVID-19
Despite previous experiences with isolation, participants from both groups found the increased social disconnection during the pandemic particularly stressful. Several participants turned to technology, such as video calls, to stay connected with loved ones. One participant noted, “Thank God for FaceTime,” while another mentioned, “My senior citizen center held Zoom meetings, which helped maintain obligations.”
Theme 5. Making Future Plans
Amid the uncertainty of the pandemic, some participants focused on future planning as a coping strategy. They expressed a desire to make the most of the present, acknowledging that “COVID made me understand the value of not putting things off” and emphasized the importance of seizing opportunities when possible.
Discussion
The study aimed to explore health disparities, which initially focused on the experiences of African American patients with cancer due to the unique emotional challenges they faced during the COVID-19 pandemic. These challenges included the political climate, the impact of the social justice movement, the murder of George Floyd, a loss of safety, and communal grief within the African American community. However, White patients with cancer were also included after expressing an interest in understanding the pandemic’s broader implications. Some White participants reflected on their fears, sadness, and a newfound commitment to activism and allyship. One participant candidly acknowledged his past bigoted attitude and described how the pandemic and witnessing George Floyd’s murder motivated him to reassess his beliefs and seek opportunities to understand others beyond racial stereotypes. Including White participants expanded the study’s scope, offering insights into shared emotional responses and differing coping strategies across racial groups.

This study also aimed to explore the experiences of both African American and White patients with cancer, providing insights into their coping strategies during this unprecedented time. The results offer valuable insights into these patients’ shared experiences while highlighting differences in their sense of belonging and optimism about the future. By examining common and distinct emotional responses, the study sheds light on how each group navigated the challenges of the pandemic, offering a deeper understanding of their coping mechanisms.
Despite African American patients’ higher physical vulnerability to COVID-19,26-28 the findings underscore the resilience and reliance on social support networks across both groups. The study suggests that further research is necessary to explore the nuances of these experiences, particularly as they relate to community belonging and coping mechanisms in different racial groups.29-31 To support participants’ resilience in coping with psychosocial, emotional, financial, and behavioral challenges during the pandemic, this study supports the role of adaptive coping strategies and social support as crucial elements in alleviating pandemic-related stressors. This study highlighted resilience as a defense that positively influenced participants’ mental well-being, allowing them to manage the complex demands of the COVID-19 pandemic. Additionally, African American participants’ specific challenges, including issues related to community integration and mistrust in medical research, suggest areas for further exploration to understand and improve coping in diverse populations.32 Both racial groups adjusted daily routines, adhered to health mandates, and maintained social connections. Both racial groups also utilized cognitive reframing, a technique that shifts one’s mindset to view situations or relationships from a new perspective.33 Participants reported that reframing their attitudes contributed to positive emotions and a sense of life satisfaction, improving their overall outlook during the pandemic. Many used their time in isolation to engage in household projects, which fostered a sense of purpose and accomplishment.

When asked to rate their current life situation on a ladder scale, African American participants reported higher average ratings than their White counterparts (8.3 vs 5.3). Similarly, African American participants were more optimistic about their future, rating their prospects 5 years ahead higher than White participants (8.8 vs 5.8). This optimism may reflect different stages of coping with cancer, as described in Kübler-Ross’s stages of grief, where African American participants may have reached the acceptance stage, while White participants appeared to be in earlier stages, such as anger or depression. The Kübler-Ross model assumes that individuals coping with a life-threatening illness such as cancer often go through these stages as part of their emotional adjustment, and this process may be influenced by both individual and cultural factors.34 However, when considering their sense of belonging to the local community, African American participants reported feeling significantly less connected than their White counterparts. This disparity might highlight the compounded stressors faced by African Americans, who often navigate not only the emotional toll of cancer but also systemic inequities and a historical lack of trust in health care systems.
This lack of connectedness may also be related to the privacy concerns expressed by African American participants, reflecting the cultural stigma around disclosing their cancer diagnosis. African Americans are often reluctant to share their diagnoses due to concerns about how others in their community may perceive their condition, as well as fears of being treated differently or stigmatized35—further influencing African American patients’ feelings of social isolation and lack of community support.
Another significant finding was the higher rate of reported deaths among African American participants’ family and friends due to COVID-19. Three African American participants reported losing close loved ones, while none of the White participants reported such losses. Additionally, contrary to previous research highlighting the importance of spirituality in African American culture, none of the Black participants mentioned religiosity as a coping mechanism during the pandemic.36 Instead, they emphasized the importance of main-taining relationships with family and friends. Notably, all African American participants accepted the COVID-19 vaccine despite the documented history of mistrust in vaccines among this population. The acceptance of the vaccine among African American participants seemed to be influenced by their personal experiences with loss, increased risk of potential death, and the belief that vaccination was necessary for survival. African American patients shared that they experienced frequent deaths from immediate family members and their communities. This compelled them to accept the vaccine despite concerns surrounding vaccine hesitancy and historical mistrust.
Study Strengths
A key strength of this study was its ability to document the coping strategies used by at-risk cancer patients as they faced the dual challenges of the COVID-19 pandemic and racial and social differences. By conducting interviews early in the pandemic, the research offers valuable insights into how participants initially responded and adjusted to the newly implemented social distancing mandates and the “new normal.” The study’s strengths also lie in the diverse age range of participants and the relevance of findings during a critical time in the pandemic. These narratives offer valuable insights into coping mechanisms and resilience, with implications for improving cultural competence, equity, and well-being for oncology patients, particularly those from marginalized communities.37
Study Limitations
The researcher identified a few recruitment challenges, particularly regarding mistrust among African American participants toward participating in the research. Although many initially showed interest, they became hesitant upon hearing the word study. The oncology social worker observed verbal and nonverbal cues indicating this mistrust, as some participants paused the interviews or asked probing questions when the word study was mentioned. This hesitation aligns with the historical and ongoing mistrust of medical research among Black communities, a sentiment rooted in events such as the Tuskegee syphilis study, which continues to influence health care participation today.38 The data in the study were also gathered from one-time interviews conducted during the early phase of the pandemic. Consequently, the researcher could not track any changes in participants’ responses to the virus that may have emerged or changed as the pandemic progressed and evolved. The study’s small sample size and narrow focus are also notable limitations. Additionally, the underrepresentation of other minority groups and participants with lower socioeconomic status limited the generalizability of the findings.
Implications for Social Work Practice
Direct Practice
Patients with cancer in this study encountered considerable social and political stressors, alongside personal losses due to the pandemic. Many participants reported losing family members, friends, and loved ones, as well as facing a decreased sense of personal autonomy and safety. Fears around mortality, cancer recurrence, and increased vulnerability due to their immunocompromised status weighed heavily on them. These experiences of grief and anxiety were shared not only by the patients but also by the care providers supporting them, highlighting that community service workers, much like family members, often similarly experience grief due to the emotional bonds formed with their patients in caregiving roles.39 This shared trauma creates a unique experience of collective mourning, affecting both social workers and patients. The profound connection established through caregiving underscores the emotional toll of loss on both parties, emphasizing the importance of acknowledging the emotional well-being of service workers in their professional roles.39
The study’s findings may help support oncology social workers and health care professionals who work with chronically ill patients in better understanding the unique stressors faced by African American and White patients with cancer in and out of the oncology treatment setting. Oncology social workers might apply more culturally sensitive approaches when engaging with marginalized groups, paying close attention to verbal and nonverbal cues, especially when encouraging participation in clinical trials or research studies. This understanding may play a crucial role in fostering collaboration and enhancing social support networks within the cancer community, ultimately improving emotional and practical assistance for patients and families. By strengthening this collaboration, individuals coping with cancer might receive more comprehensive patient-centered care and connection during their journey.
Research indicates that African American patients with cancer face additional barriers to participation in clinical trials due to historical mistrust and social inequalities, which can exacerbate stress and impact treatment outcomes.38 Addressing these disparities requires oncology professionals to be particularly aware of the influence of social determinants of health, including access to care, which often results in different emotional and practical support needs between African American and White patients.40 By recognizing and responding to these needs, oncology social workers can foster stronger relationships and trust with patients, improving support and treatment outcomes.
Social Work Supervision
Health care providers must recognize their significant impact on the quality of care in cancer centers. Oncology social workers, in particular, often find themselves burdened by the high demands of cancer care, palliative care support, and grief work, which can lead to undervaluing the profound influence they have on patients and staff. This study highlights that patients—both African American and White—rely heavily on their oncology teams for emotional reassurance, encouragement, and a sense of emotional security. Social work supervision and peer support serve as valuable outlets, offering safe spaces for discussions on race, trauma, and grief. This approach further emphasizes that social workers, like their patients, are affected by profound emotions, which sometimes challenge the traditional theories foundational to social work.41 These supportive outlets can provide paths for self-reflection, helping social workers build greater empathy and emotional awareness and fostering personal and professional growth. As Juniarta and Sitanggang noted, empathy is crucial for health care providers, including oncology social workers, as it strengthens their emotional connections with patients, fostering a more supportive and compassionate care environment.42
Concluding Thoughts
The COVID-19 pandemic posed severe risks for everyone, but its impact was significantly damaging for communities of color, a reality exacerbated by systemic inequities. As an oncology social worker and researcher, I played a dual role in this study, directly engaging with participants by conducting interviews and analyzing their experiences. My identity as a woman of color fostered a deep connection with the participants, allowing me to approach the research with empathy and cultural sensitivity. This perspective was essential in capturing the profound challenges faced by individuals navigating both a cancer diagnosis and the pandemic. By weaving my lived experiences into the study, I could better interpret the narratives shared by patients whose stories of fear, resilience, and systemic barriers resonated deeply with me. This dynamic added richness to the research and the emotional toll carried by health care workers like me during this unprecedented time. It also highlighted the delicate balance required to support others while managing my well-being. These dual roles of caregiver and researcher helped shape the study’s framework, ensuring the voices of marginalized communities were authentically represented. My involvement in earlier sections of this abstract included my role in conducting interviews, documenting narratives, and driving the analysis, as these tasks were integral to the research process.
Conducting and analyzing the research during the pandemic heightened the emotional weight of concurrent social issues, including the murder of George Floyd, which further intensified feelings of communal and disenfranchised grief for both me and the patients I worked with, pivoting across racial lines. These shared experiences of grief, fear, and resilience resonated profoundly, influencing the study’s framework and my approach to interpreting the data.
This period underscored the broader conversation about racial inequities in health care, aligning with the call to action by Lori J. Pierce, MD, FASTRO, FASCO, then president of the American Society of Clinical Oncology, who urged that the fight against racism should be approached with the same commitment and focus as the fight against cancer itself.43
Lisa Petgrave-Nelson, DSW, LMSW, OSW-C, is a certified oncology social worker, a trained end-of-life doula, and an NYU Zelda Foster Palliative Care and Leadership Fellow. With over 20 years of experience, her roles have encompassed caring for patients in acute inpatient and outpatient nephrology and oncology settings, including Emory University Hospital, Cancer Treatment Centers of America, and her current position at The Cancer Institute at St. Francis Hospital.
Acknowledgments
I am profoundly grateful to the patients who took part in this study, most of whom, sadly, have since passed away. Their bravery and willingness to share such personal and challenging experiences will always be honored and remembered. I also extend my heartfelt thanks to my family, colleagues, mentors, oncology team, and friends for their unwavering support and guidance during the study’s distribution and analysis phases. A special acknowledgement goes to Eugene Rubach, MD, FACHS, whose simple yet timely phone call helped steer me in the right direction with the IRB process. His thorough and perceptive data analysis left me in awe and with profound gratitude. Deep appreciation goes to Carolyn Messner, DSW; Susan Gerbino, PhD, MSW, the late Esther Chakas; Lailea Noel, PhD, MSW, FACCC; Eucharia Borden, LCSW; and Mohia Basu, MPH, for their meaningful insights and contributions to this study.
References