Author(s):
The Centers for Medicare & Medicaid Services (CMS) released proposed rules for the calendar year (CY) 2026 Medicare Physician Fee Schedule (MPFS) on July 14, 2025, and the Hospital Outpatient Prospective Payment System (HOPPS) on July 15, 2025. Although both rules were shorter in length than in previous years, they were significantly denser in proposed changes to payment policies.
MEDICARE PHYSICIAN FEE SCHEDULE1
Payment Rates
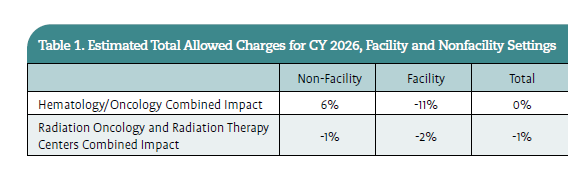
Beginning in CY 2026, as required by section 1848(d)(1)(A) of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA),2 there will be 2 separate conversion factors (CFs): 1 for items and services provided by a qualifying Alternative Payment Model (APM) participant; and another for other items and services provided by a nonqualifying APM participant. The conversion factor is a value set each year that converts the relative value units (RVUs) of physician work, practice expense, and malpractice of each code and their geographic locations into the assigned CMS payment rate; it is determined by building on the CF from the preceding year. The update for CY 2026 to the APM qualifying CF is 0.75%, resulting in an estimated increase of $1.24 (3.82%) from the CY 2025 CF. The update to the nonqualifying APM CF is 0.25%, resulting in an increase of $1.17 (3.62%) from the CY 2025 CF. CMS estimates the CY 2026 PFS qualifying APM CF to be $33.5875 and the nonqualifying APM CF to be $33.4209. Note: even though the conversion factors are each proposed to increase next year, which should result in positive adjustments to payments, 2 payment adjustments that CMS is proposing would nullify many of these increases. Table 1 shows the estimated per total allowed charges for CY 2026.

Proposed Efficiency Adjustment
CMS again expressed concern that—as physicians become more proficient—there is no accountability for gains in efficiency for non– time-based services. In other words, services that physicians perform daily or repeatedly throughout their practice are expected to take less time, become less complex, and require less mental and physical effort. Ultimately, this efficiency gain would result in a decrease in the physician work RVUs and payment for the service. Additionally, there are many codes that the AMA/Specialty Society RVU Update Committee (RUC) has never valued: 5382 of 9970 codes have never been valued by a RUC survey. Finally, even after a code is surveyed, it may take 2 to 3 years before the values go into effect.
In 2018, the Medicare Payment Advisory Commission (MedPAC), an independent legislative branch agency that provides Congress with analysis and policy advice related to Medicare, recommended 3 options to Congress to address these CMS concerns:
1. An automatic reduction to the prices of new services and services with high growth rates
2. An extension of the annual numeric target for CMS to reduce the prices of overpriced services
3. An across-the-board reduction to all fee schedule services other than ambulatory evaluation and management (E/M) services.
For CY 2026, CMS proposed that an efficiency adjustment be applied to physician work RVUs and intraservice time for all non–time-based services paid under the MPFS. CMS indicated the proposal is based on the “assumption that both the intraservice portion of physician time and the work intensity (including mental effort, technical effort, physical effort, and risk of patient complications) would decrease as the practitioner develops expertise in performing the specific service. As expertise develops, learning leads to enhanced familiarity with the various aspects of a service, variations in the anatomy of each patient, and confidence in the practitioner’s own ability to handle unexpected challenges that arise.”
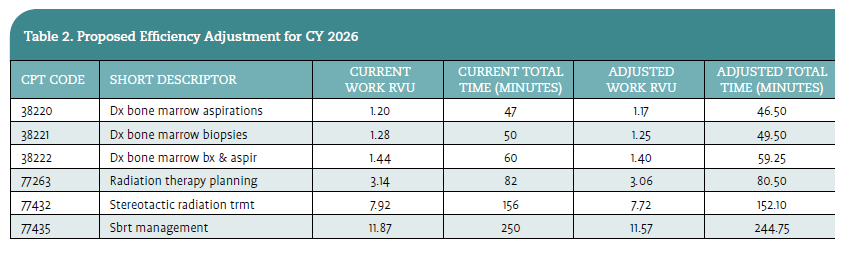
CMS proposed implementing the efficiency adjustment by decreasing the work RVUs and the intraservice physician time for codes describing non–time-based services by a factor equal to the Medicare Economic Index (MEI) productivity adjustment. The efficiency adjustment uses a lookback period of 5 years of productivity adjustments, resulting in a 2.5% total decrease applied to baseline physician work RVUs and intraservice time values for CY 2026.
For oncology, the impact would not be significant for hematology/oncology, as most services billed by these physicians are time-based services (ie, E/M and drug administration). Radiation oncologists perform E/M, but the bulk of their services are not time-based; this accounts for the projected 1% decrease overall and for nonfacility settings. To see what these proposed changes might look like, Table 2 provides a look at select oncology-specific codes. CMS has made available the full table of services impacted by this adjustment online.

CMS has proposed applying the efficiency adjustment every 3 years. If finalized, the next update would be applied in CY 2029 and reflect efficiencies gained during the years 2027-2029. This timeline would align with timed updates to the Geographic Price Cost Index (GPCI) and the Malpractice (MP) RVUs, which also occur every 3 years.
CMS is soliciting comments on the proposed initial look-back period of 5 years for the efficiency adjustment, and the use of MEI productivity adjustment percentage values for calculating the efficiency adjustment for CY 2026. CMS is specifically seeking comments on whether adjustments should be made in future rulemaking, and importantly, whether efficiencies should stop accruing for services after a predefined number of years.
Proposed Site-of-Service Payment Differential
Over the past several years, CMS has addressed the shift in practice ownership from physicians to hospitals. CMS reported in 1988 that 72% of physicians were full or partial owners in their respective practices. In 2024, data supported that a dramatic decrease had taken place, where only 35.4% of physicians fully or partially owned their practices. This change was not the result of practice closures, but rather a shift in ownership to hospitals acquiring physician practices. The agency reports that physicians in hospital-owned practices have increased by over 47% between 2014 and 2024.
For CY 2026, CMS proposed a payment adjustment designated as a site-of-service payment differential. This proposed adjustment is intended to address the potential and belief that there is a duplicative payment for practice expense (PE) incurred by physicians working in the facility setting (ie, hospitals and ambulatory surgical centers). Practice Expense in the office (nonfacility) setting accounts for and values the cost of supplies, equipment, and staff for each service. When the physician provides services in the hospital or ambulatory surgical center (facility) setting, there is some practice expense that is valued for the physician. Typically, this value may be for more indirect expenses, not resources directed to the individual patient, but to maintain their practice while working in the hospital. However, with more physicians employed by and/or working in the facility setting, most, if not all practice expenses are covered by the hospital. MedPAC raised this concern in their 2018 report to Congress: “In cases when clinicians practice exclusively or almost exclusively in a facility, or where a facility is financing indirect PE for clinicians, payment to both entities for indirect PE costs may be duplicative and unnecessary.”3
The proposed site-of-service payment differential will be calculated by reducing the portion of the PE RVUs allocated to the physician for performing the service in the facility setting by half of the amount assigned to the indirect PE RVUs in the nonfacility setting. The site-of-service payment differential will impact physicians practicing in the facility setting more than those in the nonfacility setting. It is meant to remove any duplicative valuation of services and better balance physician payments between facility and nonfacility settings.
For oncology, specifically hematology/ oncology, this area is where the greatest impacts are estimated. As mentioned earlier, time-based services are the predominant services billed by hematology/oncology as opposed to radiation oncology. The proposed decreases in services in the facility setting will negatively impact E/M visits. CMS estimates a decrease of 5% to 10% to the overall reimbursement for E/M visits. When combined with any other services billed by hematology oncologists, this proposed change results in an estimated 11% decrease in reimbursement for CY 2026. The magnitude of the impact on hematology/oncology will depend on the practice patterns and specialty of any given physician; it does not mean every hematology oncologist will see the same reductions.
Specific Codes and Code Set Valuations
Within the CY 2026 proposed rule, CMS addressed multiple misvalued and/or proposed value changes to a specific series of new and established Current Procedure Terminology (CPT®) codes. CMS explains that its rationale for the proposed changes is based on values recommended by the RUC and other organizations that CMS utilizes for assistance in setting appropriate values for codes. Radiation will be impacted the most by the proposed CY 2026 coding changes, with an overhaul of the external beam treatment delivery codes in both the facility and nonfacility settings.
Radiation Oncology Treatment Delivery
CMS introduced significant updates that will substantially impact radiation oncology, particularly freestanding practices. One of the most notable proposals is the shift in how CMS calculates PE values for services like treatment delivery. Rather than relying on PE inputs from the RUC, CMS has proposed to use audited HOPPS data to recalibrate the PE for technical services, including those commonly used in radiation therapy.
At the September 2024 CPT Editorial Panel meeting, the panel approved the revision of CPT codes 77402, 77407, and 77412 to establish a technique-agnostic family of codes with imaging guidance bundled into the 3 codes, and the deletion of CPT codes 77385, 77386, and 77014. These services were subsequently reviewed by the RUC, and a valuation recommendation was submitted to CMS for inclusion in CY 2026 rulemaking. Although CPT codes (77402, 77407, 77412, 77385, 77386, and 77387) were established for CY 2015, CMS has not used them for payment under the MPFS in the freestanding center, only in the hospital setting. In 2015, CMS identified concerns with the packaging of Image Guided Radiation Therapy (IGRT) into some of the treatment delivery codes in the family and not others. As a result, CMS created 17 HCPCS G codes, mirroring the existing codes (at the time), maintaining CPT code 77014, and establishing values that linked directly to the existing values/inputs for the MPFS.
For CY 2026, CMS proposed deleting these 17 G codes and assigning values to the newly revised CPT codes for payment under the MPFS, in conjunction with the proposal to utilize HOPPS cost data to establish PE RVUs, as previously described. CMS also proposed utilizing the relationship between the proposed HOPPS ambulatory payment classification (APC) relative weights for APCs 5621, 5622, and 5623 to determine the valuation of PE-only CPT codes 77402, 77407, and 77412 when paid under the MPFS.
To align the MPFS payment for this code family with the HOPPS payment, CMS proposed assigning Procedure Status “B” to the technical component of CPT codes 77387 and 77417 to maintain consistency with the HOPPS payment for this code, which is bundled into payment for the treatment delivery codes, and not separately billable. While this change would be appropriate for the external beam treatment delivery codes, it would negatively impact proton therapy centers.
If CMS moves forward with bundling all imaging guidance technical components, proton therapy centers would not be able to recoup monies for the imaging technology they purchase and utilize, even though guidelines allow for billing. The definitions of proton treatment delivery: 77520 (Proton treatment delivery; simple, without compensation), 77522 (Proton treatment delivery; simple, with compensation), 77523 (Proton treatment delivery; intermediate), and 77525 (Proton treatment delivery; complex) do not include imaging guidance within the definitions, nor within the direct PE values of the codes. Therefore, it would be appropriate for imaging guidance, 77387-TC and 77417, to be reported by the office-based proton center for the imaging guidance performed at the time of treatment delivery. Additionally, AMA guidance of the coding changes for CY 2026 highlights that the technical component of imaging guidance (CPT code 77387) is billable with proton treatment delivery codes.
Superficial Radiation Treatment
Superficial radiation therapy and electronic brachytherapy are currently provided using CPT codes 0394T (High dose rate electronic brachytherapy, skin surface application, per fraction, includes basic dosimetry, when performed) and 77401 (Radiation treatment delivery, superficial and/or ortho voltage, per day) in conjunction with CPT code 77280 (Therapeutic radiology simulation-aided field setting; simple) and HCPCS code G6001 (Ultrasonic guidance for placement of radiation therapy fields). In October 2020, HCPCS code G6001 was identified by the Relativity Assessment Workgroup screen via the CMS/ Other Medicare utilization of over 20,000.
In January 2021, the RUC recommended referring G6001 to the CPT Editorial Panel to develop new code(s) that reflects the different processes of care between the 2 specialties (dermatology and radiation oncology). After a 2-year delay to allow time for re-review, in September 2024, the CPT Editorial Panel created 4 codes and a new subsection to report surface radiation therapy. These codes will replace CPT codes 0394T, 77401, and HCPCS code G6001.
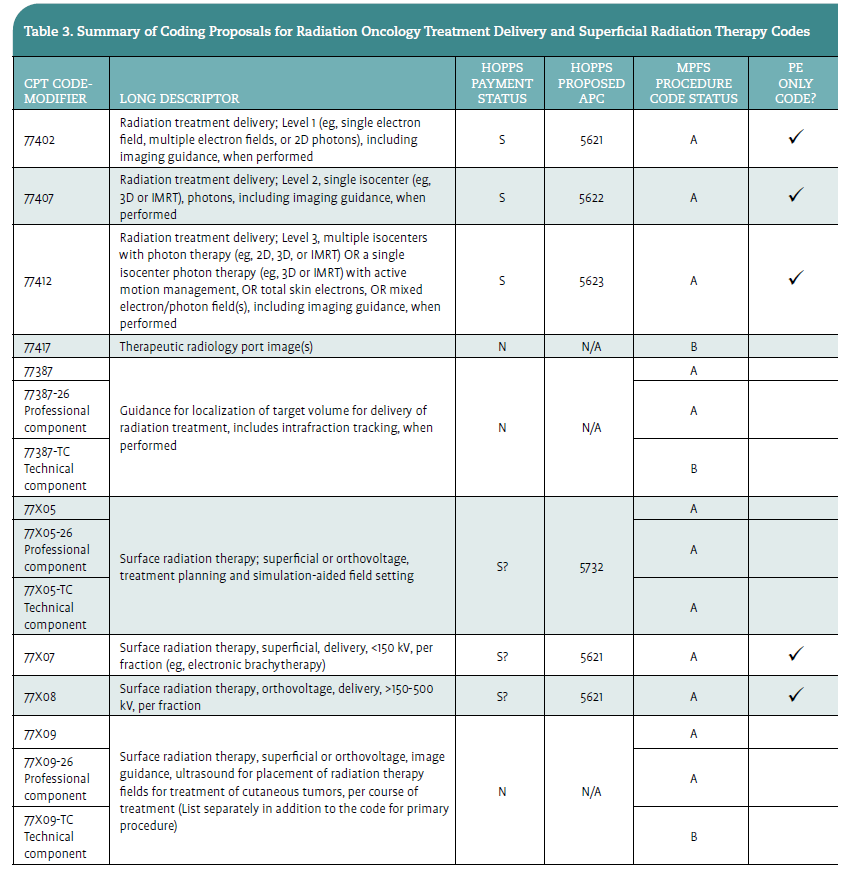
CMS proposed the RUC-recommended work RVU for the 2 codes in the family that have work RVUs assigned. CMS also proposed utilizing APCs 5621 and 5732 to determine the valuation of PE-only CPT codes 77X07 and 77X08 and the technical component of CPT code 77X05. To maintain alignment between the MPFS and HOPPS payments for this code family, CMS proposed to assign Procedure Status “B” to the technical component of CPT code 77X09 to align with the packaging of the code into the treatment delivery CPT codes 77X07 and 77X08. CMS did propose displaying CPT code 77X09 in Addendum B with the professional and technical components, where the technical component is nonpayable under Procedure Status “B,” as well as the global service equal to the payable professional component.
CMS provided Table 3 to assist in better understanding the code and payment status regarding the updates for CY 2026 for both external beam radiation and superficial radiation therapy.

Proton Beam Treatment Delivery
The MPFS payment amounts for proton beam treatment delivery services are contractor-priced and currently determined by local Medicare Administrative Contractors (MACs). CMS has not previously established RVUs for these services due to the unique nature of the equipment costs associated with these services. Given the proposals described above to establish RVUs for the new and revised CPT codes for Radiation Oncology and Superficial Radiation Treatment Delivery Services, CMS is seeking comments on whether to establish RVUs for proton beam treatment delivery services or if there is some other method that would be more appropriate. These services are assigned to APCs 5623 and 5625 under the HOPPS, with established Medicare payment rates (unlike the contractor pricing that is in place for these services under the MPFS).
Scalp Cooling Services
At the September 2024 CPT Editorial Panel Meeting, the 2 current Category III codes (0662T and 0663T) were deleted, and 3 new Category I codes were created:
1. 9XX01: Mechanical scalp cooling, including individual cap supply with head measurement, fitting, and patient education)
2. 9XX02: Mechanical scalp cooling; including hair preparation, individual cap placement, therapy initiation, and precooling period)
3. 9XX03: Mechanical scalp cooling; provided after discontinuation of hemotherapy, each 30 minutes [List separately in addition to code for primary procedure]).
The new codes were surveyed as part of the January 2025 RUC meeting. The codes do not have any physician work; these are practice expense-only services.
CMS did not agree with the RUC-recommended 5 minutes of clinical staff time for 9XX01. Instead, the agency recommends 27 minutes, based on the reference code. CMS accepted and proposed all the other RUC-recommended PE inputs for the family without modification.
Payment for Telehealth Services
CMS currently utilizes a 5-step process for determining services on the Medicare Telehealth Services List. This process involved categorizing each service as permanent or provisional status rather than 1 of the 3 categories. A service was assigned provisional status if there was not enough evidence to determine the service provides clinical benefit to the patient, but there was enough evidence to suggest further review may show the clinical benefit.
Beginning with the CY 2026 Medicare Telehealth Services List, CMS proposed to revise the 5-step review by removing steps 4 and 5 for clarity purposes. Under this proposal, services on the Medicare Telehealth Services List would no longer be designated permanent or provisional. All services listed or added on the Medicare Telehealth Services List would be considered included on a permanent basis.
CMS would still reserve the right to remove services included on the Medicare Telehealth Services List based on internal review or feedback received from interested parties. If finalized, all codes currently on the list (provisional or permanent) will remain on the Medicare Telehealth Services List. Because CMS has already determined that services with a provisional designation satisfy the standards represented in Steps 1 through 3 in prior rulemaking cycles, it does not believe further review would be required to justify their inclusion on the Medicare Telehealth Services List under the revised process. This includes CPT code 77427 (Radiation treatment management, 5 treatments), which is proposed to be maintained for use with real-time audio/ video capabilities.
Physician Supervision of Residents in Teaching Settings
In previous rule making, CMS established a policy that allows teaching physicians to fulfill supervision requirements to be present for the key or critical portions of services through audio/video real-time communications technology, when services are provided by a resident. This policy was only valid for services furnished in residency training sites that are located outside of an Office of Management and Budget (OMB)–defined metropolitan statistical area (MSA). This distinction was made to increase beneficiary access to Medicare-covered services in rural areas.
CMS again expressed concerns that continuing to permit teaching physicians to bill for services furnished involving residents when they are virtually present, outside the conditions of the PHE (public health emergency) for COVID-19, may not allow the teaching physician to have personal oversight and involvement over the management of the portion of the case for which the payment is sought. Therefore, CMS believes that permitting Medicare payment to continue for this PHE flexibility is no longer necessary.
Under this proposal, for services provided within MSAs, physicians must maintain physical presence during critical portions of all resident-furnished services to qualify for Medicare payment, not just in-person services, ensuring consistent oversight standards.
The proposed rule to not extend flexibilities for virtual services would not impact teaching physicians’ ability to provide virtual supervision of residents for educational purposes. Teaching physicians retain the discretion to provide greater involvement in resident-furnished services and may determine when virtual presence is appropriate based on the specific services and the experience level of the residents involved.
Social Determinants of Health Services
Prior to 2006, a primary focus for CMS was related to equity in and access to care and how social determinants of health (SDOH) impact the ability to diagnose or treat the patient. As part of these efforts, CMS established coding to improve payment accuracy for additional time and resources dedicated to helping patients with serious illnesses as they navigate the health care system or remove health-related social barriers. After further review of utilization information, CMS believes the resource costs described by HCPCS code G0136 (Administration of a standardized, evidence-based social determinants of health risk assessment tool, 5 to 15 minutes) are already accounted for in existing codes, including but not limited to E/M visits. Therefore, CMS proposed deleting this code for CY 2026. Accordingly, CMS proposed removing this code from the Medicare Telehealth Services list.
Physician Practice Information Survey
The AMA introduced the Physician Practice Information Survey (PPIS) in 2007 to collect data on direct and indirect practice expenses incurred by physicians in their practices. Initial data were collected through a comprehensive survey process for inclusion in the MPFS rate setting process for CY 2010. The updates were incorporated over a 4-year transition period, replacing previous data sources. Since that time, CMS has sought comments on how to best update the data and collection methodology.
The AMA completed the PPIS and Clinician Practice Information (CPI) survey at the end of 2024 and shared the results with CMS ahead of the February 10 deadline for inclusion in the upcoming rulemaking cycle. The agency’s initial review of the AMA data reflects several concerns related to accuracy, utility, and suitability to replace the current PE/HR data for payments under the MPFS. CMS outlined in more detail some of its concerns:
• Low response rates and representativeness
• Small sample sizes and sampling variation
• Lack of comparability to previous survey data
• Potential measurement error
• Missing and incomplete data submission.
Due to these concerns, CMS did not propose implementing the PE/HR or cost shares from the AMA’s survey data for CY 2026. Instead, CMS proposed maintaining the current PE/HR and 2006-based MEI cost shares for CY 2026 MPFS rate setting. The file, CMS-1832-P_ PEHR_063025, was included in the addenda for CY 2026 MPFS proposed rule; it outlines the PE/ HR by specialty.
HOSPITAL OUTPATIENT PROSPECTIVE PAYMENT SYSTEM4
Payment Rates
CMS used the CY 2024 claims data for rate setting for CY 2026, which follows the usual 2-year difference in data for rate setting to allow for 1 year of timely filing for billing. CMS proposed a 2.4% increase to the outpatient departments (OPD) fee schedule. Based on the market update from the Inpatient Prospective Payment System (IPPS) of 3.2% and a 0.8% productivity adjustment decrease, this results in a proposed conversion factor (CF) of $91.747 for hospitals that meet the Hospital Outpatient Quality Reporting requirements. After applying a 2% reduction rate, hospitals that do not meet these requirements will have a CF equal to $89.958.
CMS estimates total payments to HOPPS providers will be approximately $100.0 billion, which is an increase of approximately $8.1 billion compared to CY 2025 HOPPS payments. CMS proposed an increase of 2.4% to payment rates for ambulatory surgical centers (ASCs) that meet the quality reporting requirements under the Ambulatory Surgical Center Quality Reporting Program.
Cancer Hospital Payment Adjustment
For CY 2026, CMS proposed continuing the additional payments to cancer hospitals utilizing a payment-to-cost ratio (PCR) factor. CMS proposed a target PCR of 0.87 to determine the cancer hospital payment adjustment to be paid at cost report settlement, which includes the 1.0% reduction.
Procedures Assigned to New Technology APC Groups
When new technology is assigned a billing code, it can be difficult for CMS to establish a payment rate difficult because there are no claims data to determine utilization and cost by the hospital. Once there are sufficient data, the new technology is moved to a clinically appropriate APC. Consistent with current policy, for CY 2026, CMS proposed to retain services within the new technology APC groups until sufficient claims data are received to justify reassignment to a clinically appropriate APC. This policy provides flexibility to reassign a service to a clinical APC in less than 2 years if sufficient claims data are received. One new technology specific to radiation oncology is Biology-Guided Radiation Therapy (BgRT).
Biology-Guided Radiation Therapy
BgRT uses positron-emitting radiopharmaceuticals to control the delivery of radiation therapy to treat primary and metastatic lung or bone tumors. Effective January 1, 2025, HCPCS codes C9794 and C9795 were replaced by HCPCS codes G0562 and G0563, respectively. For CY 2026, the proposed HOPPS payment rates are based on available CY 2024 claims data. There are no CY 2024 claims for HCPCS codes G0562 and G0563 since they were not effective until CY 2025. However, as HCPCS codes C9794 and C9795 were still in use until December 31, 2024, CMS proposed determining the payment rate for HCPCS codes G0562 and G0563 using the available claims data for HCPCS codes C9794 and C9795.
For CY 2026, CMS proposed to designate HCPCS codes G0562 and G0563 as low-volume procedures under the universal low-volume APC policy, given there are only 16 claims for C9794 and 28 claims for C9795 during the claims period. CMS proposed to assign HCPCS code G0563 to APC 1525 (New Technology-Level 25 [$3501-$4000]) with a payment rate of $3750.50 for CY 2026. CMS proposed to perform a similar analysis using updated claims data in the CY 2026 HOPPS/ASC final rule.
Payments of Drugs, Biologicals (including Biosimilar Products), and Radiopharmaceuticals
Each year CMS assesses payments for drugs and biologicals based on current pricing methodologies, which includes payments for drugs and biologicals considered separately payable based on the assigned APC or pass-through status. For CY 2026, CMS proposed to continue the current payment policy in effect from CY 2013. The few items in which CMS is proposing new policy or payment include:
• CMS proposed to continue to package drugs and biologicals estimated at a per-day administration cost less than or equal to $140; this maintains the current CY 2025 value.
• CMS proposed to continue paying for qualifying biosimilar products with an average sales price (ASP) less than the reference biological ASP, for a calendar quarter during an applicable 5-year period, at ASP plus 8% of the reference biological ASP. Biosimilars are exempt from the threshold packaging policy when their reference biologicals are separately paid. These biosimilars will also be paid for separately, even if their per-day cost is below the packaging threshold.
Payment for Diagnostic Radiopharmaceuticals
Historically, diagnostic radiopharmaceuticals have been packaged into the imaging service they are performed with and are not paid separately. CMS has done this for multiple reasons, the primary being the agency believes packaging policies are an inherent principle of the HOPPS. However, CMS also feels strongly about ensuring availability of new and innovative diagnostic services for beneficiaries. For 2026, CMS proposed to pay separately for any diagnostic radiopharmaceutical with a per-day cost greater than $655; this amount is an increase from the current value of $630. Any diagnostic radiopharmaceutical with a per-day cost less than $655 would continue to be packaged under the current policy. Within the addendum payment files, diagnostic radiopharmaceuticals that exceed the proposed threshold of $655 have been assigned a status indicator “K” for easy identification.
Proposed Change to 340B Drug Discount Program Remedy
Historically, the 340B Program aimed to provide safety-net hospitals (hospitals serving low-income, uninsured, and Medicaid patients) that qualified as covered entities the opportunity to purchase outpatient medications at discounted prices. Drug companies were required to offer 340B hospital discounts to be able to participate in the Medicaid program. After significant litigation, the previous payment policy was reversed, and drugs purchased under the 340B program were again paid at ASP+6%, and CMS is required to repay monies when the policy was to pay ASP –22.5%.
In the Final Remedy Rule, CMS applied a 0.5% reduction in the HOPPS conversion factor applicable to nondrug items and services, excluding hospitals that enrolled in Medicare after January 1, 2018. CMS finalized the start date of this policy for CY 2026, stating the 0.5% reduction would be in effect until the payment reduction reached the estimated $7.8 million, which CMS estimated would be in CY 2041.
For CY 2026, CMS proposed to revise the annual reduction to the HOPPS conversion factor from 0.5% to 2%. CMS expects this revised reduction rate to reach a total offset of $7.8 million in approximately 6 years, rather than 16 years. As stated in the Final Remedy Rule, this reduction would not apply to new providers. CMS also proposed that the CY 2026 HOPPS payment rates that used rate setting under the ASC payment system would not include the 2% offset to the HOPPS conversion factor.
Drug Administrations Furnished in Excepted Off-Campus Provider-Based Departments (PBDs)
According to a 2023 MedPAC report, chemotherapy services furnished in OPDs have increased from 35.2% in 2012 to 51.9% in 2021.5 CPT code 96413 (Chemotherapy administration, intravenous infusion technique; up to 1 hour, single or initial substance/drug) is one of the most frequently billed drug administration codes. According to CMS, when reviewing the assigned rate for 96413, $199.36 (national rate) in the office setting vs $331.69 (national rate) in the outpatient hospital setting, the difference is roughly 178% higher in the facility setting than in the office setting. CMS expressed concern not only for the impact on the Medicare program, but to Medicare beneficiaries and their cost share of being treated in the outpatient hospital setting.
CMS indicated that it was also concerned that the drive to treat more patients in the PBD setting is due to this financial incentive. Most services are reimbursed at a higher rate in the outpatient hospital (facility) setting than in the office (nonfacility) setting. To address what CMS believes are issues with the same services performed in a setting that would financially benefit the provider, the agency proposed to establish a payment policy to ensure site neutrality.
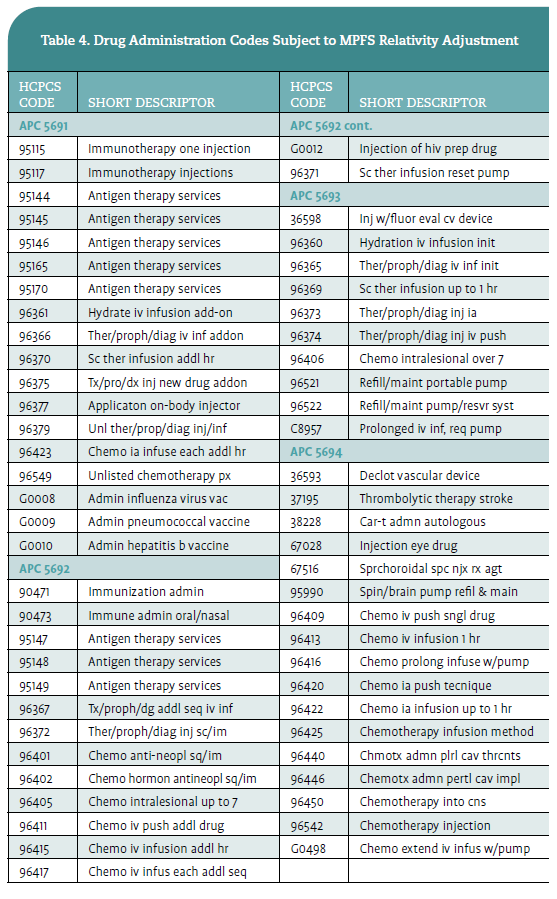
For CY 2026, CMS proposed to apply the MPFS relativity adjustment to drug administration codes within APCs 5691, 5692, 5693, and 5694 as they currently do for clinic visits (G0463). Meaning, the excepted provider-based departments would no longer be paid at the full HOPPS rate; instead, they would be paid at 40% of the rate, a reduction of 60%. CMS believes this change would align reimbursement to that in the office-based setting and be paid under the MPFS. Table 4 includes all drug administration codes within the selected APCs proposed by CMS to be paid at 40% of the HOPPS rate.

Comments for both the MPFS and HOPPS proposed rules were open to stakeholders until 11:59 pm EST September 12, 2025, and 11:59 pm EST September 15, 2025, respectively. Stakeholders were able to submit comments electronically or by mail, with electronic submissions encouraged via http://www. regulations.gov.
The final rules for MPFS and HOPPS are expected on or before November 1, 2025. Stay tuned to Oncology Issues to learn what payment policies and regulatory updates were finalized as proposed or something different.
Teri Bedard, BA, RT(R)(T), CPC, is executive director of Client and Corporate Resources at Revenue Cycle Coding Strategies in Des Moines, Iowa.
References
1. Medicare and Medicaid programs; CY 2026 payment policies under the physician fee schedule and other changes to Part B payment and coverage policies; Medicare shared savings program requirements; and Medicare prescription drug inflation rebate program. Federal Register. Published July 16, 2025. Accessed August 28, 2025. https://www. federalregister.gov/documents/2025/07/16/202513271/medicare-and-medicaid-programs-cy-2026payment-policies-under-the-physician-fee-schedule
and-other
2. Medicare Access and CHIP Reauthorization Act of 2015. Accessed August 28, 2025. https://www.govinfo. gov/content/pkg/PLAW-114publ10/html/PLAW114publ10.htm
3. Report to the Congress: Medicare Payment Policy. Medicare Payment Advisory Commission (MedPAC). Published March 2018. Accessed September 17, 2025. https://www.medpac.gov/document/http-wwwmedpac-gov-docs-default-source-reports-mar18_ medpac_entirereport_sec_rev_0518-pdf/
4. Medicare and Medicaid programs: Hospital outpatient prospective payment and ambulatory surgical center payment systems; Quality reporting programs; Overall hospital quality star ratings; and Hospital price transparency. Federal Register. Published July 17, 2025. Accessed August 28, 2025.
https://www.federalregister.gov/documents/2025/ 07/17/2025-13360/medicare-and-medicaid-programshospital-outpatient-prospective-payment-andambulatory-surgical
5. Aligning Fee-for-Service Payment Rates Across Ambulatory Settings. Medicare Payment Advisory Commission. Published March 2023. Accessed September 17, 2025. https://www.medpac.gov/ wp-content/uploads/2022/07/Site-neutral-March 2023-SEC.pdf