Author(s):
Oncologists suffer from high levels of compassion fatigue and burnout. In the past, levels ranged from 35% to 45%.1 More recently, in a 2023 survey, 59% of oncologists reported 1 or more symptoms of burnout; 57% reported high levels of emotional exhaustion; 34% reported they “have become more callous” toward people.2 The financial toll is estimated to be up to $4.6 billion per year due to costs associated with physician turnover, physician shortages, and absenteeism.3 The COVID-19 epidemic, the increased requirement to see more patients, the loss of physician autonomy, long working hours, more time spent completing the electronic health record (EHR), structural racism, institutional and gender bias (including in compensation), and the exposure to frequent patient deaths all contribute to burnout.1-4
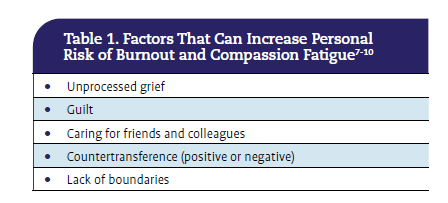
Mitigating factors for oncologists discussed elsewhere focus on recognizing the importance of physician well-being and providing support for the practice, administration, patient care, and staffing.1,3,4,5 Strategies to build resilience, inclusion, and visibility in an organization also improve fatigue and burnout and promote professional satisfaction.3-6 Yet, the important contributions of unprocessed grief and countertransference have received less attention in oncology literature, though they are well recognized as important in psychiatric and psychological practice and palliative care (Table 1).7-10

Feelings of Grief
Oncologists have seen it many times: adult children weeping in the exam room; nurses tearful after saying goodbye for the last time to a beloved patient who is going to enroll in home hospice. As oncologists, we offer our support and that of our staff.
Some data indicate that oncologists prefer guilt to helplessness.15 It may feel less bad to be guilty, since one is blaming oneself for failing
the patient and can strive to do better next time; helplessness is less amenable to reversal. These feelings can lead clinicians to withdraw from patients they know are dying, or perhaps to visit them less frequently in the hospital, to protect themselves.13
We know the classic Kubler-Ross stages of grief that our patients and families will manifest: denial (“It’s someone else’s CT scan!”); anger (spouses or partners attacking you for “not caring” when you delivered bad news); bargaining (“I’ll do anything if you enroll me in the next trial”), depression; and (in some cases) acceptance (Table 2).11

Grieving oncologists also manifest these stages. They may experience intuitive grief with feelings of sadness, crying, and loss of sleep. Or, perhaps more likely, they may have instrumental grief, manifested not by crying, but by the need to do something.12 Instrumental grief is triggered by thoughts of lost patients and rarely includes crying or the need to talk about the patient who has died.11 It may be impossible to tell that an instrumental griever needs support. But if a colleague is avoiding usual social contact, seems to have a shorter temper, or seems more distractible, they may be grieving.
Qualitative interview studies reveal the additional components of oncologists’ grief, which include fiduciary duty to patients and feelings of responsibility for patient outcomes that cause feelings of powerlessness, guilt, self-doubt, and failure.13 That grief can spill over to their home life, and oncologists may distance themselves from loved ones.12 Caring for patients who are personal friends or colleagues induces even more anxiety, difficulty defining boundaries, and emotional exhaustion.14
Many among us have experienced these feelings. Some of us may be unconsciously going through the stages of grief now, especially the denial stage, which leads to compartmentalization and bargaining.13 Psychologically, it is less painful to obsess over what other choices we could have made or which other treatments might have worked better than to face our raw helplessness over the disease’s progression and our patients’ deaths. Some data indicate that oncologists prefer guilt to helplessness.15 It may feel less bad to be guilty, since one is blaming oneself for failing the patient and can strive to do better next time; helplessness is less amenable to reversal. These feelings can lead clinicians to withdraw from patients they know are dying, or perhaps to visit them less frequently in the hospital, to protect themselves.13 An oncologist’s grief is lonely. Stanislav Lazarev, MD, a radiation oncologist at Icahn School of Medicine in New York, recently wrote: “What lingers is not just the grief but also a profound sense of isolation. You want to share your feelings…but finding an outlet can be challenging. Your colleagues, as compassionate as they may be, often have their own patients and concerns. You hesitate to burden them. At home, you grapple with the decision to bring this sadness into your family’s life. As a result, the grief remains contained, swirling in a quiet space that offers no easy relief.”16 That was certainly my experience throughout most of my career.
Dysfunctional Strategies for Grieving
In fact, I devised several strategies over the years to process my grief, first as an oncologist and later as a palliative care and supportive care clinician caring for patients with cancer. I was a woman physician in the years when we made up less than 10% of the physician workforce, at a time when there was significant concern about our ability to withstand the rigors of medicine. So while I was an intuitive griever, visibly crying was out of the question for me.
My first strategy as a house officer (resident physician) was fairly primitive: I found a stairwell where, between patient visits, I could cry unseen. That solution was not foolproof, but it worked most of the time. Later, as a first-year oncology fellow, I was allowed only to care for patients with advanced-stage disease who were not eligible for studies. Of course, I lost many more patients than I had as a house officer. But there was no one to discuss this with. I decided that instead of looking for stairwells, when the lights dimmed at a concert, I would reflect on my patients who had died. After several months of this, I said to my husband, “Let’s not go to the symphony tonight. I don’t have the energy to cry.” He, a poet, was understandably confused. Only after I explained to him my system of evoking each patient in turn, grieving them, and then moving on to the next, did I realize how dysfunctional that solution was.
Disenfranchised grief, however, can occur when a person’s loss is not openly acknowledged, socially validated, or publicly mourned.17 Oncologists and their team members who knew and worked with a patient closely, often for years, are not expected to grieve openly.
After abandoning that practice, I did my best to grieve as the occasion arose, during the workday, the drive home, or the following weekend. I thought I had my grief down pretty well, but unbeknownst to me, my subconscious had concocted another scheme that protected and healed me. I became aware of it only this year when, on a flight from London to Boston, I found myself crying bitterly; I recalled all the other flights on which I had done something similar. The sky had become my safe place, my new stairwell where no one knew me, and I was free to cry to my heart’s content. I have flown almost a million and a half miles, for work and for pleasure, and most of that time I was working or reading or watching films. And I did not consciously choose to grieve; it just happened when it needed to, overflowing my resistance and the barriers I had created to keep the grief in check. I wonder whether, since I’m aware of it now, that solution will still work. I’ll redouble my efforts to grieve in the moment. But I also need to recognize when I must postpone those feelings, because the next patient and family need me, and try to ensure I make time to grieve later that day.
Maybe making a note to myself will work. I have a mindfulness calendar that reminds me twice a day to breathe. Maybe a biweekly reminder, grieve, will work as well.
Experiencing Disenfranchised Grief
Culture determines who is entitled to grieve a loss. Spouses, parents, grandparents, children, and close friends and coworkers are generally enfranchised, that is, expected to show signs of grief.
Disenfranchised grief, however, can occur when a person’s loss is not openly acknowledged, socially validated, or publicly mourned.17 Oncologists and their team members who knew and worked with a patient closely, often for years, are not expected to grieve openly.
These providers may take a few hours to attend the wake or the funeral, but they are not expected or encouraged to take days off for bereavement. These providers are not offered condolences, and their distraction and distress are rarely acknowledged. Deaths of patients for whom they had countertransference (see below), of long-term patients or young people, and unexpected deaths, as well as unrealistic expectations of the patient’s family (eg, about a cure or the physician’s responsibility for their loved one’s death) or high family needs all contribute to oncologists’ unresolved grief.18
Implications for Oncologists
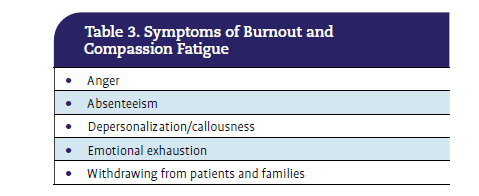
Oncologists and their teams may not even realize that they are entitled to grieve. When grief remains unprocessed, there is often nothing left for the next patient or family.13 Disenfranchised grief leads to compassion fatigue and all the symptoms of burnout, such as anger at work or at home, absenteeism, feelings of depersonalization (ie, lacking empathy toward patients or anger at patients), and emotional exhaustion (Table 3). Oncologists may find themselves making rounds at the hospital in the early morning hours, before the family arrives, to avoid the extra pain those encounters can cause.

I wonder how many of my oncology colleagues share this lack of space, time, and ritual for grieving. I wonder if they even feel entitled to grieve, and if so, where and with whom? The literature does not provide answers, yet this may be one of the most important issues to address if compassion fatigue is to be prevented.
Delaying Palliative Care Consultations
Oncologists may feel they have failed a patient when they have no more therapies to offer against the cancer. Although intellectually, these providers know that it’s medicine’s failure, not their own, that’s not what it feels like. Guilty feelings and unconscious pangs of grief can make it hard to tell patients that they are at the end of treatment. These feelings also make it difficult to recommend that the time has come to focus on making the most of their remaining time or to recommend that patients change goals to optimize their quality of life and alter their code status to do not resuscitate/do not intubate (DNR/DNI).
Palliative care colleagues are happy to provide the support oncology teams need, but unprocessed memories of painful experiences of partnering with palliative care in the past, along with unrecognized subconscious feelings of grief, guilt, failure, and helplessness may deter oncologists from referring to palliative care, as making that referral may mean admitting they failed.15,19,20
Personal Solutions
Deferral, such as the compartmentalization I mentioned above, can be a very effective coping strategy if used carefully. A more effective way for clinicians to heal from their losses is to reach out to social support networks or engage with the activities and people associated with one’s faith. Other coping strategies include practicing self-care (eg, sleep, nutrition, exercise), processing grief, and forgiving oneself. Identify the activities needed to maintain physical, emotional, and spiritual health, and commit to engaging in them. It may be helpful to find someone to share the feelings of guilt, helplessness, and hopelessness that will invariably arise. Forgive yourself and acknowledge that you did the very best you could.
Anecdotally, the TV show Shrinking (Apple TV) offers a simple practice: rather than try to suppress feelings of grief, allow yourself to grieve fully just for the length of a favorite song and follow that by engaging in vigorous activity. Repeat as often as needed.
Interpersonal Solutions
To begin to process grief, share it with colleagues, meet with the family, make condolence calls, or send a card.21 Inform nurses and social work colleagues about your preferences for support when your patients are not doing well to help with anticipatory grief and whatever transpires at the end of their care. ASCO’s Well-Being Task Force created a pilot oncology group-peer-support virtual program supported by trained peer facilitators.5,6 The biweekly, 2-hour resilience training program took place over 3 weeks; it improved physician well-being, and the 15 participants (11 of whom completed all the sessions) reported high levels of overall satisfaction with it.
Organizational Solutions
Some surgeons use morbidity and mortality rounds to replace rumination. They answer their what-ifs, explore their guilt, and label bargaining as a useful learning from experience. If managing an oncology program or leading a practice collaboratively, establish a top-down expectation that grief is a natural part of the work and requires regular attention, ensuring time and space for staff to address grief. Staff can normalize discussing tough cases that cause them to “play the tape over and over in their heads.” Airing the distress and allowing the rational mind to explore irrational feelings enables people to “put those feelings away” and make way for the sadness, acceptance, and forgiveness they deserve.
Establish an office bereavement program that automatically sends materials at specified times after patients’ deaths. Include information about normal grief and how oncology staff might offer help for bereaved families.22 Hold a remembrance service at regular intervals, so that clinical and administrative staff can take time to grieve patients they have known.23
Transference and Countertransference
What do these psychiatric terms have to do with oncology? We are not therapists. Our job is to provide state-of-the-art therapy for our patients and to treat the adverse effects of those therapies. Our oncology care teams expect and can treat anxiety. We recognize depression and demoralization, and we rely on our social work, spiritual care, psychiatry, and palliative care colleagues to help patients and families with these issues. Therefore, understanding patient transference and recognizing our own countertransference were not part of our formal medical or oncology training. Yet, these are key elements of the therapeutic relationships upon which successful patient treatment and outcomes depend.
Transference refers to how patients feel about us, ie, the “repetition of feelings, attitudes, and behaviors attached to early formative relationships in the context of a therapy relationship.”9 While psychological therapy is usually what is meant, cancer treatment also qualifies as “a therapy relationship.” According to Noorani and Dyer: “The power imbalance in this relationship between a patient in need and a clinician looked to for help can revive patients’ memories of relationships with earliest caregivers and elicit powerful feelings of love, hate, longing, and dependency. This is especially important in the oncology setting, where illness and disability can threaten patients’ autonomy, self-esteem, and self-control, leaving them feeling especially vulnerable.”9
Disenfranchised grief, guilt, and unrecognized countertransference contribute significantly to the development of compassion fatigue and burnout among oncologists. Oncologists must recognize that they have not failed when their patients die; medical science has failed.
A large part of the transference, therefore, is about how much we or our actions remind patients unconsciously of positive or negative experiences in their past.7,8 Consider these scenarios: Harold, a 55-year- old man with stage III colon cancer, has followed your instructions meticulously and praises you at each visit. But when his disease recurs, he is furious with you and accuses you of incompetence and not caring. If you knew that Harold’s parents had promised him unending success if he just followed the rules, and his life until his cancer diagnosis had been pretty perfect because he did, you might be able to take his attacks less personally.
Suzanne, a 25-year-old woman with metastatic breast cancer, always seems aloof and guarded. You might have expected this reaction during a first visit, but she never seems to warm up to you, though she gets along well with her infusion nurses. You may unconsciously remind Suzanne of her stepmother, who did her best to “replace” Suzanne’s mother after her mother died when Suzanne was 5 years old. Suzanne has always resented her. But who is likely to have this information? With an understanding of transference, we could take a step back, reflect on what was happening with Harold and Suzanne, and reach out to our social work and nursing colleagues to help us unravel the story. Without this understanding, however, our day would be ruined; we are likely to take Harold’s accusations of betrayal and worthlessness and Suzanne’s rejection to heart. With enough of these encounters, compassion fatigue and burnout follow not far behind.24
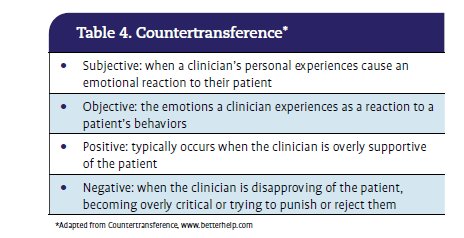
Countertransference is even more insidious. Countertransference is a psychological phenomenon in which clinicians unconsciously allow their personal feelings toward patients to dictate what those patients need (Table 4). Countertransference can be positive or negative. It is expected, normal, and will happen. It should not be a source of shame. It is the natural consequence of being a human caring for a human, and our medical knowledge does not mitigate countertransference. But if it goes unrecognized, countertransference can lead to both substandard care for the patient and burnout for the oncologist.

Countertransference occurs when something about a patient unconsciously reminds us of a relative, a teacher, or even a former lover. We unknowingly react to them as we did to the person in the previous relationship. Consider this scenario: when Cassandra, a woman of my mother’s age and temperament, asked me to do things I would not normally do when treating a patient (eg, allowing her to skip lab check-ins that were inconvenient), I found myself acquiescing, though I did not know why. I knew there was a risk, but it was what she wanted. This was an example of a positive countertransference, in which I found myself having an unusual attachment to the patient because she had so many of the same attributes as my mother. Other similarities might include treating someone who is close to your age, ethnic identity, gender expression, or background (eg, both being of the same faith or a child of immigrants).19
I gave Cassandra my cell number, letting her know I’d be there for her even when I wasn’t on service. This is termed a boundary crossing.8 Boundary crossing is a major component of burnout for clinicians who do it often because they feel that’s what they owe their patients. If clinicians understood why they felt this sense of obligation, they would be less likely to make these offers, more consciously protect their private time, and suffer less often from burnout.
Oncologists may unconsciously try harder to save patients for whom they have positive countertransference and find themselves falling into deeper despair when these patients die. Unaware of why they feel this way, oncologists may go the extra mile to find a phase 1 trial for the patient and are crushed when their efforts fail. These oncologists find it difficult to have conversations about a poor prognosis and DNR/DNI choices even when the patient has advanced disease that is no longer responding to therapy and may have only weeks to live.
Negative countertransference is similarly destructive. Consider this scenario: Mr. Nash unconsciously reminds you of your disparaging and brutal physical education teacher. You dread seeing his name on your visit list, though if asked, you could not say why. Although you have nothing difficult to discuss with him this week, you are likely unable to do a complete assessment and be fully present for this patient. You feel helpless and hopeless after each visit. Because Mr. Nash senses this, he fails to provide key information about his recent treatment-related diarrhea, which results in him being hospitalized for dehydration later that week.7
Avoiding the Pitfalls of Countertransference
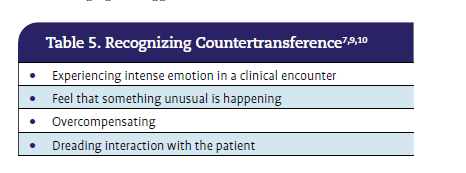
How can oncologists recognize when countertransference is at play (Table 5)? Bapat and Bojarski state: “Whenever a clinician experiences intense emotion during a clinical encounter, be it pleasant or unpleasant, this may signify the presence of transference and/or countertransference.”10 Rosenberg et al recommend: “We can offer ourselves ‘internal supervision’ and take a few moments for introspection of our emotional state when something feels unusual or intense in a clinical situation. [We can ask] am I doing things to overcompensate my reluctance to see her, such as exceeding the usual appointment time?”7 Ask yourself what seemed unusual or surprising, and talk with a colleague about what happened. It is normal to have a variety of responses to patients, but try to explore what in yourself may have been triggered by this patient.9 Acknowledging the triggers can defuse them.

Ask the patient, as well. Consider how they perceive you, what has triggered them, or what assumptions they may be making based on their previous experiences with people “like you.”
Talk with a social worker or a palliative care colleague about encounters that feel unusual, emotionally charged, or painful. Consider asking them to meet with the patient to unpack what triggered the transference in the patient or the countertransference in the oncologist.
Recognize the factors within yourself that can trigger positive or negative countertransference, and partner with palliative care or office staff when seeing such patients. Feelings for a young mother, for instance, may cause you to spend more time than necessary in her room, affecting the schedule and the efficiency of the infusion room for the whole day. Negative feelings toward a demanding, entitled matriarch may cause enough frustration that maintaining a professional stance becomes difficult. In these cases, it may be beneficial to avoid meeting with these patients alone.
Anticipate a greater likelihood of frustration or anger when caring for patients who trigger strong emotional responses. Extra time may be needed for errands or getting to the airport, difficult conversations with colleagues may need to be postponed, and tasks requiring more patience should be delegated. It may be helpful to ask partners to supervise homework or bedtime on days when your emotional energy is particularly taxed.
Concluding Thoughts
Disenfranchised grief, guilt, and unrecognized countertransference contribute significantly to the development of compassion fatigue and burnout among oncologists. Oncologists must recognize that they have not failed when their patients die; medical science has failed. Accepting help to acknowledge and process grief—whether recognized by others or not—and grieving together with staff and colleagues can facilitate healing. By partnering regularly with social work and palliative care teams, oncologists can better identify signs and symptoms of countertransference in themselves or their colleagues and choose to replace helplessness with constructive coping rather than guilt. The more oncologists explore these pervasive influences on their practice, unearth the reasons, recognize the potential dangers, and partner with supportive colleagues, the more likely they will be able to maintain joy in their work and avoid the pitfalls of compassion fatigue and burnout.
Janet Abrahm, MD, FACP, FAAHPM, FASCO, is a professor of medicine at Harvard Medical School in Boston, Massachusetts and a member of the Division of Adult Palliative Care in the Department of Supportive Oncology at Dana-Farber Cancer Institute in Boston, Massachusetts.
References










")

: Not Traditional Telehealth Services")



















