FROM 2010 TO 2019, the Association of Cancer Care Centers (ACCC) fielded an annual Trending Now in Cancer Care Delivery survey to its membership to gain insights into issues faced and—most importantly—solutions to address those issues. When its busy provider members shared the challenges involved in completing this time- and resource-intensive survey, ACCC identified alternative ways to collect these data, including at the ACCC Annual Meeting & Cancer Center Business Summit (AMCCBS). Beginning in 2023, ACCC hosted a series of interactive sessions on hot topic areas impacting oncology and the delivery of cancer care. Insights and solutions from discussions at AMCCBS 2025 were used to develop this report: 2025 Trending Now in Cancer Care: Part 1. Look for 2025 Trending Now in Cancer Care: Part 2 in the next Oncology Issues. Prior reports are available on the ACCC website.

Facilitators
This 2025 AMCCBS deep dive session built on the 2023 deep dive, which level-set and defined the concepts of AI and BI, and the 2024 deep dive, which explored the power and promise these technologies hold for care delivery, providers, and patients with cancer. “Today’s session is less about theory and more about execution,” Dr. Flora said at the start of the 2-hour discussion. “As we talk around the country on these topics, the same questions come back again and again. How do I get started? Who’s doing this? How do I pick a tool? Do they really work as well as people say they will? With our presentations today, you’re going to get a better understanding of how AI and BI can be applied in your clinics, in your offices, and in your hospital systems.”
ROI on an AI Solution in Early Lung Cancer Detection
Amie Miller highlighted the significant impact of AI in early lung cancer detection. At the Brian D. Jellison Cancer Institute, AI tools are used to identify incidental pulmonary nodules from CT scans, which are often missed. The AI system scans radiology reports for key words and anatomical locations, enabling the early detection of potential malignancies.
“When people initially thought about early lung cancer detection, they thought about it as a loss leader—mission driven. There wasn’t a whole lot of consideration that early lung cancer detection could generate substantial revenue for your health care system,” Miller said. “So that’s one of the things I’m going to talk about today, and I’m going to hone in on how AI helps us do that.”
Sarasota Memorial Health Care System started with a lung cancer screening program but ultimately came to the realization that the hospital was missing an opportunity to catch lung cancers earlier with an incidental pulmonary nodule program. When developing this program, Miller advised that lung cancer screening and incidental pulmonary nodule programs need to work in tandem to develop a standardized process first to identify and then manage these patients, using evidence-based tools like the Fleischner Society guidelines to minimize patient risks and detect disease in its earliest stage.
She then described the typical journey of an incidental lung nodule patient. “Patients come into the emergency department [ED] for, let’s say, a car accident. They have a CT of the abdomen and pelvis, looking for internal bleeding, and then the CT happens to capture a left lower lobe pulmonary nodule.” While radiologists accurately report those incidental nodules, patients are often discharged from the ED without the patient or their primary care physician being made aware of the nodule or next steps. “Unfortunately, 18 months, 2 years, or even 5 years later, these patients are coming in with late-stage disease,” said Miller.
And that’s where AI comes in. AI solutions have the ability to scan radiology interpretation reports and pick out key words, the anatomical location, and the size of the nodule so that it can be risk stratified. Moreover, AI works seamlessly behind the scenes, without additional burden on its human radiologist counterparts. “There’s no change to our workflow. Our radiologists don’t do anything differently. They’re still documenting and interpreting the reports,” shared Miller. “But now our AI platform is also looking at the reports, scanning through them to identify the information and data needed to pull into an incoming work list and automatically triage patients according to risk status.”
Miller stressed that it is important to understand that while lung cancer screening and incidental lung nodule programs save lives, they also generate revenue for the health care system. “To those of you on the business side trying to make a case to your CFO, COO, or service line leaders, these programs are a way that clinicians can save lives at scale,” shared Miller. “Another ROI [return on investment] consideration is that these programs also generate referrals to the cardiovascular service line, because AI can also find cardiac calcifications.” Bottom line: AI technology finds additional incidental elements that may need follow-up from health care providers—not just pulmonary nodules.
Key Points
BI Technology to Help Manage Workflow and Treatment Schedules in Radiation Oncology
Liz Hyde discussed how Oklahoma Cancer Specialists and Research Institute, a free-standing, for-profit, physician-owned practice, implemented oncology-specific analytics software to address staffing shortages, support staff workflows, and reduce the burden of labor-intensive manual data tracking. Specific to managing workflows and treatment schedules in radiation oncology, the Mosaic analytics tool used by this practice provides detailed reports on:
Labor Management
BI tools track staff performance and workload distribution, ensuring efficient use of resources. For example, all dosimetrists at Oklahoma Cancer Specialists and Research Institute work remotely. With BI tools, the cancer program can show that these remote staff are as efficient—if not more efficient—than when they worked in clinic “because they don’t have a physician walking into the dosimetry lab and they’re not getting called to the machine when they don’t necessarily need to be called to the machine,” shared Hyde. The same is true for physicists. “There is a large shortage of physicists, so we do not want to overwork the physicists we have,” explained Hyde. “We need to make sure that their work is evened out [balanced], and we’re able to do that with these tools.”
Treatment Statistics
Real-time data on patient treatments and procedures help in budget planning and operational efficiency. “This report helps me see where I am on a weekly basis and adjust staffing accordingly,” Hyde said. BI tools can run retrospective and prospective patient volume reports. “One of my favorite reports is the weekly number of patients treated,” shared Hyde. “This report is not the number of patients scheduled but the number of patients who received treatment.” These reports provide an overview across all radiation oncology locations and allow management to compare patient volumes, patient starts, treatment regimens, and equipment use. “This report goes into my email every Monday morning at 4:00 am, so when I get to work, it’s there for me to review,” said Hyde. And if one location is trending down, data can be mined to determine a cause(s). “When I’m doing a budget review, I can say that this location had to close due to weather and it affected the budget.”
Downtime Analysis
BI tools can run downtime reports to help leadership understand how this will impact revenue and budgets. Identifying and addressing barriers to treatment continuity, such as patient no-shows, improves overall care delivery. “We were able to cut our downtime patients in half just by having the data and working with our social work team,” Hyde shared. Specifically, this heightened focus led to a decrease in patient no-shows from 636 (2%) to 339 (1%), which is a significant recoup of lost revenue. Oklahoma Cancer Specialists and Research Institute also participated in the national quality improvement initiative, Breaking Barriers, aimed at reducing missed radiation therapy appointments (no-shows) to improve access to high-quality oncology care, particularly for diverse communities and care settings. With these data, the practice was able to determine root causes behind patients missing treatments and in 2024 achieved the goal of zero patients missing treatment for controllable reasons.
Patient Demographics
As part of its participation with the Breaking Barriers initiative, Oklahoma Cancer Specialists and Research Institute focused on its patients with head and neck cancers, as well as breast cancers. “We knew that it [no-shows] wasn’t going to be a real problem for our breast cancer patients. They’re usually excited to get started on treatment. They want to get everything taken care of,” said Hyde. Patients with head and neck cancer face significant side effects and are “less willing to come into treatment.” Hyde explained, “They’re usually younger, and sometimes their social status [social determinants of health] are not as good as other patients. So, there are a lot of factors that keep them [patients with head and neck cancer] from being able to come in and get their treatment.” To address these challenges, the radiation oncology team worked with the social service and nutrition teams to develop these solutions:
Patient Treatment Processes
Oklahoma Cancer Specialists and Research Institute uses its BI tool to track simulations scheduled against the number completed; these data support better equipment planning and labor management. Other treatment-related processes tracked:
Hyde shared a specific example, “Say our data show that it is taking 14 days for patients to get started [on radiation oncology treatment], and we don’t think it should take that long. We then ask: Where is the gap; where is the problem? And I don’t know if you guys are surprised, but most of the time the issue is the contouring times.” With BI data that identify and then define these types of issues, the practice can develop quality and process improvements, increasing patient, clinician, and staff satisfaction, streamlining patient throughput, and increasing revenue.
Program Growth and Market Trends
BI tools provide predictive analytics for future treatment trends, helping with budget planning for staffing and equipment. Specifically, these reports can show the volume of work that is possible, so that cancer programs can ensure they have adequate staffing to carry out that volume of work, Hyde explained. “This report will trend the next couple of years on where they think you will be,” Hyde explained. For example, BI data revealed that while the cancer program’s 3D planning had gone down, SBRT (stereotactic body radiation therapy, which treats tumors outside the brain and spine) and SRS (stereotactic radiosurgery, which targets tumors within the brain and spine) had gone up. “And because SBRT and SRS both use precise, high-dose radiation delivered in fewer treatments than traditional therapy, you would expect those trends,” said Hyde. “We can also break data out by physician,” continued Hyde. “So, if we have a physician that, for whatever reason, is not hyper-fractionating breast patients at the same level as others, that’s information I can provide for our physician leaders to discuss and determine why they feel that’s happening.”
BI tools can also support efforts to increase market share. Hyde highlighted the importance of understanding patient demographics to improve care delivery and marketing strategies. “When you understand where your patients came from before and why these patients are not coming now, you can develop strategies to market to those areas you’ve lost,” Hyde explained. In addition to heat map data comparisons to determine where volume is growing and declining, Oklahoma Cancer Specialists and Research Institute is looking at trends by diagnosis type to better target its marketing efforts.
Finally, BI tools have been instrumental in helping the practice prepare for and operate within alternative payment models, providing compliance-ready data aggregation and real-time patient tracking.
In closing, Hyde emphasized the importance of maintaining good relationships with vendors to optimize the use of BI tools. “Keeping your vendor relationships close and collaborating with vendors to make needed changes is crucial,” she advised.
Leveraging AI to Increase Clinical Trial Enrollment and Streamline Processes
Clinical trials move cancer treatment forward. “The NCCN [the National Comprehensive Cancer Network] says that the best thing for any patient in oncology is to be enrolled in a clinical trial,” Dr. Maher stated at the start of his presentation. “Unfortunately, we’re only putting about 5% of people on trials nationally, even though 70% of people have expressed interest.” Maher went on to outline 4 barriers to clinical trial accrual: lack of trained personnel; access to clinical trials; legal, regulatory, and operational processes that slow activation of clinical trials; and identification of appropriate patients—with the last challenge being the one he focused on.
Dr. Maher said there are basically 4 ways cancer programs identify patients who are appropriate for clinical trials. The first is to continue use of manual processes. “And let’s just put an X through that option,” he stated, because manual processes are resource-intensive and require more dedicated personnel and time than most community cancer programs can afford.
The second option is to leverage capabilities within the electronic health record (EHR), for example, Slicer Dicer, a data exploration, analytics, and reporting tool within the Epic EHR, that “requires resource and time-intensive manual inclusion and exclusion criteria analysis.” Maher shared an example of how to use Slicer Dicer to identify patients with PALB2 variants for the PRIORITY study. While the EHR can “export a list of those patients, a human being would still have to manually come back in and look at all those individual patients.”
A third option is use of third-party solutions like TrialGPT, Deep 6 AI, and MassiveBio, among others.
And then there’s the solution TriHealth Precision Health Institute chose: use of third-party hybrid trials where “we’re bringing the trial to our patients, rather than sending the patient somewhere else.” TriHealth’s integration with Tempus occurred in 2020, with the adoption of its program Tempus TIME, a just-in-time trial network that leverages data, technology, and a network of site partners to accelerate patient enrollment and open trials. “Tempus TIME incorporates central IRB, master agreements, and AI to allow [trial] activation in 2 weeks,” said Dr. Maher. A core component of the Tempus TIME program is AI TApp, software that uses patient data, trial eligibility criteria, and natural language processing models to match patients to suitable clinical trials, facilitating patient screening and enrollment. Integrating with EHR data, AI TApp provides real-time alerts and patient matching, increasing trial participation. “AI kept track of all changes and updates, making the process much more efficient,” Dr. Maher noted.
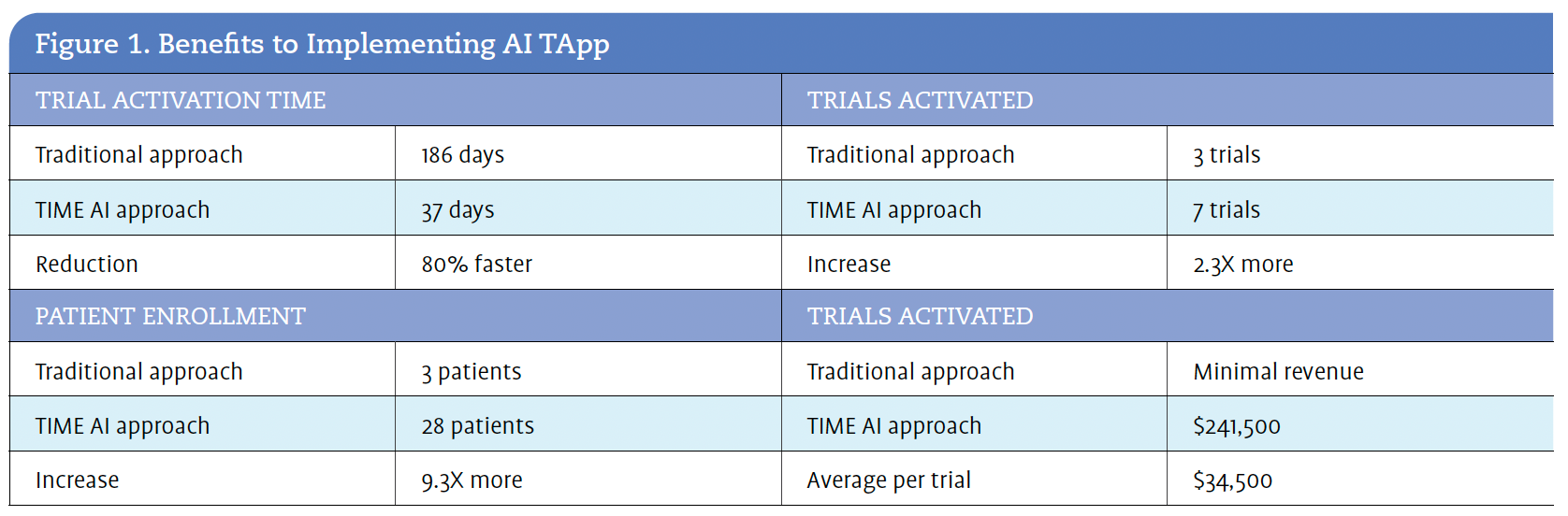
Over a 15-month hybrid trial, AI TApp conducted more than 8.6 million unique searches for 135 Tempus TIME trials across 18,823 TriHealth patients. During this time period, trial eligibility changed 985 times; There were more than 200,000 clinical updates, and AI kept up with all of those changes. The hybrid trial made 2032 potential matches (1944 interventional and 88 observational) for 45 different clinical trials. Next, Tempus AI nurses spent 389 hours reviewing those 1944 interventional matches before sending 284 patients to TriHealth providers for evaluation. Figure 1 outlines the benefits TriHealth realized with this AI approach.
So, what did TriHealth do with those 284 patients? “These patients came as a generated ‘watchlist’ that we reviewed at our molecular tumor board,” explained Dr. Maher. After sharing a screenshot of the watchlist, Dr. Maher continued. “We also have 2 molecular-based CRCs [clinical research coordinators] who monitor these patients, facilitate enrollment, and stay on top of changes.”
TriHealth has now launched about 5 different chimeric antigen receptor (CAR) T-cell trials, which require a lot more integration, also through AI TApp. “This has increased the interest of [trial] sponsors,” said Dr. Maher. “TriHealth has now had 3 or 4 [clinical trial] sponsors come to us because of the number of patients we have enrolled through this AI solution.
By integrating AI tools with its EHR, TriHealth has streamlined the identification of eligible patients for clinical trials, significantly increasing enrollment rates by 24%. Use of AI has also allowed TriHealth to see a return on its investment, with substantial revenue generation and improved patient access to cutting-edge treatments. “We gained $240,000 in that [15-month] time period, averaging about $35,000 per patient,” Dr. Maher shared.
Harnessing AI Across the Continuum of Cancer Care
Nicole Centers outlined the transformative ways that AI and BI can help cancer care teams and oncology programs:

“AI can help us in a lot of ways. It can help us streamline our programs. It can help us not have to keep hiring staff just because there’s more work to do. It can help us understand patient trends. It can also help us develop more robust programs that our providers can engage with, and our nurses can feel a part of,” said Centers. “But when it comes to real-world implementation, you can’t boil the ocean. You have to do it one drop at a time.”
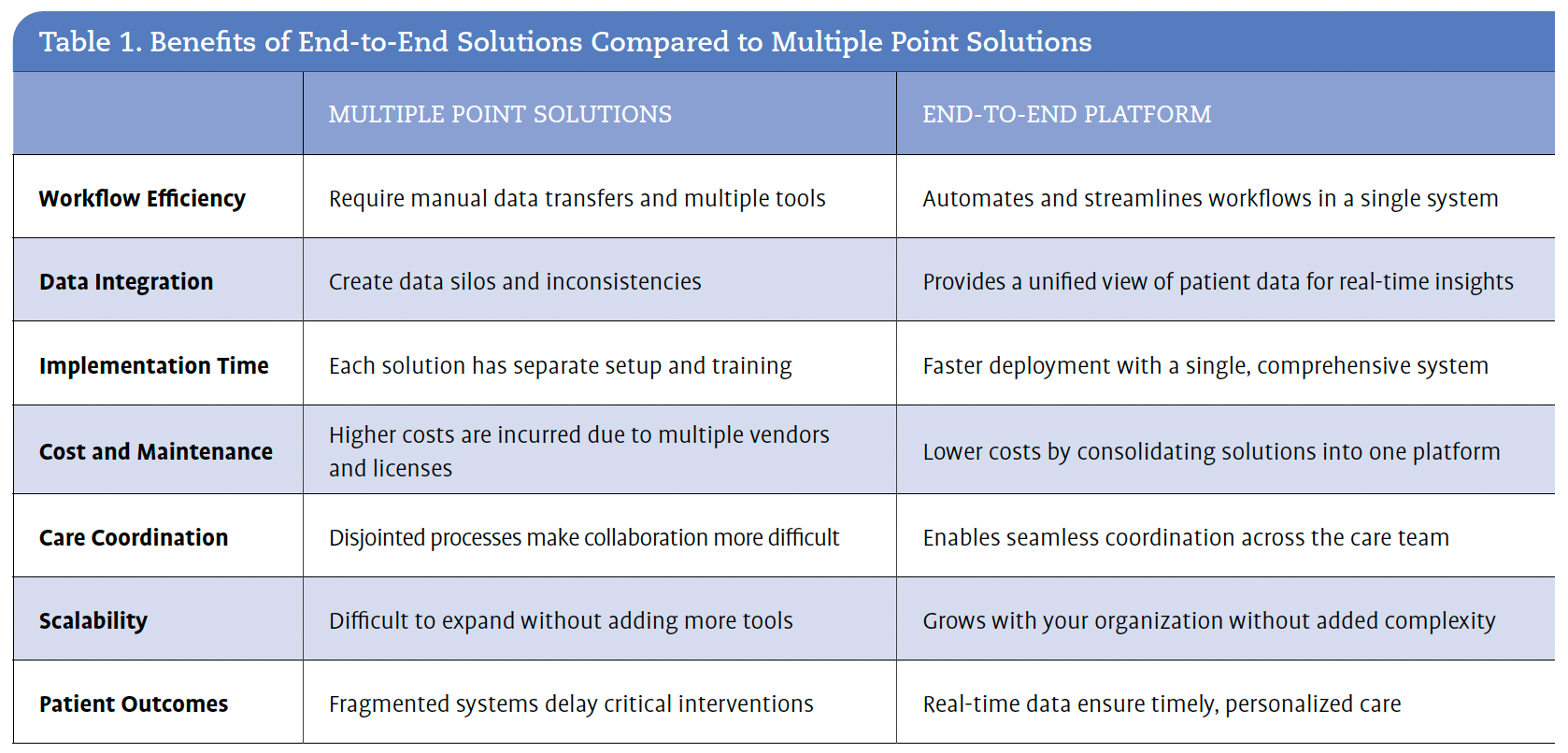
For a complex health care system like Wellstar Health System, which must meet the needs of many different stakeholders—including clinicians working chairside, registrars working remotely, and members of the C-suite—consolidating multiple tools into a single platform was key. Centers noted that Wellstar moved from multiple smaller contracts to a few broader, end-to-end contracts to simplify its operations. “We had lots of contracts with lots of people to do lots of niche things. We’re now in the process of having 1 main contract and maybe 1 or 2 smaller ones, so that we can improve data management and streamline processes and workflows,” she explained. Table 1 outlines the benefits that Wellstar identified for implementing an end-to-end solution over multiple point solutions.
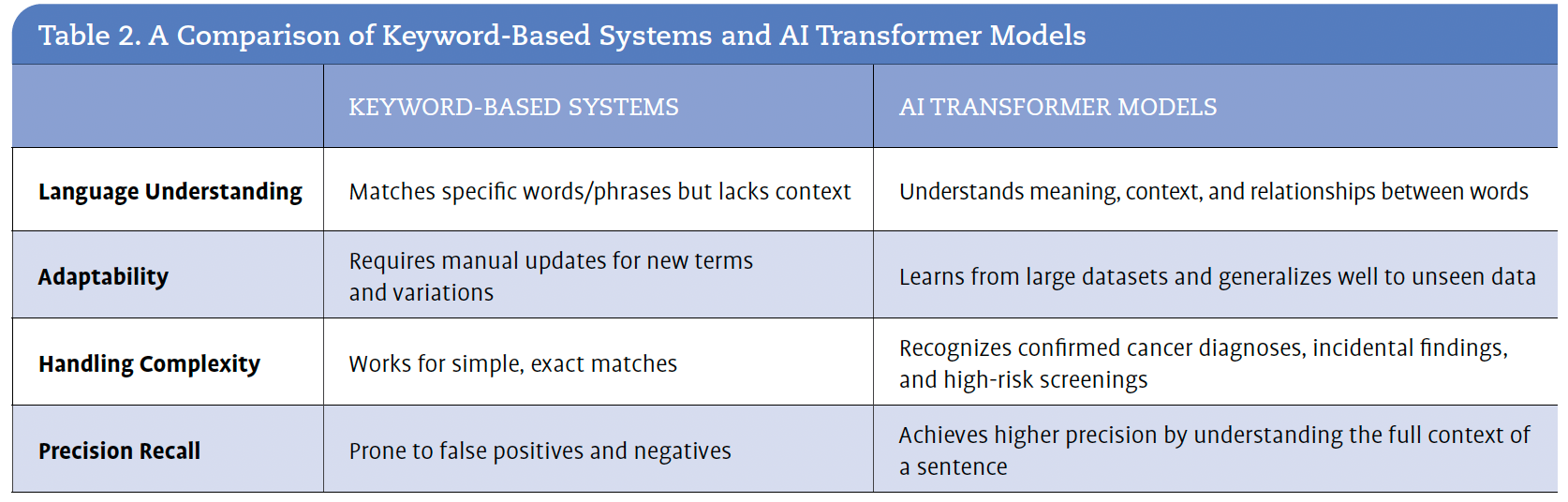
In a marketplace inundated with tools and solutions, Centers suggests that another key element to consider in the decision-making process is whether to use a keyword-based system or an AI transformer model. Centers explained that transformer models analyze unstructured data in radiology and pathology reports in real time. They also allow navigators to see a prioritized queue of confirmed cancer patients, suspicious incidental findings, and high-risk screenings. Table 2 outlines the benefits that Wellstar identified when implementing an Al transformer model. For Wellstar, the impact has been an:
However, implementing AI was not without challenges. Centers recounted how outdated manual processes and contracts initially hindered progress. Wellstar faced a significant setback when a government contract for an IT software tool related to the SEER program was not renewed, leading to unexpected six-figure costs. “But that’s when Wellstar learned that we don’t have to react. We can be proactive in our decisions,” she said, describing how the health care system evaluated various vendors and ultimately chose Azra AI for its ability to automate and improve efficiency in registry, navigation, and tumor board management.
Another selling point for Azra AI was its approach to learning and working with clients. During Wellstar’s evaluation process, most vendors, when asked about the reliability of their tool or solution, would provide a number—whether that number was 95% or 97% or 99% reliability. “I went to Azra AI, and they said, ‘What’s your tolerance?’ And I responded that while I’m a perfectionist, I never let perfect get in the way of good,” shared Centers. “And so, we [Wellstar and Azra AI] were able to set the tolerance as we went. We had a higher degree of specificity. We also had more erroneous reports because we were learning as we kept refining the tool to what works best for us and for our teams.”


Centers went on to say that she liked “working with a company that understands you’re trying to fix things as you go and can be creative in finding solutions.”
The real-world impact and the significant ROI achieved through the implementation of AI tools at Wellstar have been substantial. Centers explained how these tools have streamlined processes and improved staff productivity. “The AI tool told us how much time it was able to save us. My request for 3 additional FTE [full-time equivalent] cancer registrars was no longer necessary because AI was able to automate so many fields,” Centers explained, emphasizing the cost savings from reduced staffing needs.
The AI tools have provided valuable insights into patient volume and staff productivity. Centers shared, “We can show patient volume. We can show [the] number of patient encounters. We can show time spent with patients.” These automated reports have allowed Wellstar to better understand and manage its resources, ensuring that patient care remains efficient and effective. The ability to generate detailed reports quickly has been a game changer, enabling the organization to make informed staffing decisions, optimize its operations, and focus more on patient care rather than administrative tasks.
Centers shared that these AI tools have also reduced the Wellstar IT department’s workload. “Our IT department loves that it’s not having to work with 4 and 5 different vendors anymore,” she noted.
Looking to the future, Centers outlined several goals for enhancing Wellstar’s AI capabilities with plans to improve tumor board automation, integrate more automated fields from the EHR, and develop predictive analytics. Additionally, Centers expressed a desire to improve patient engagement with AI, envisioning a future where patients can interact with these tools to help track their data and care. “I want to see a way [forward] to where patients can engage with this technology.”
Implementation of AI presents its own set of challenges, however, including contract negotiations. “The contracting process is painful at every health care system,” she noted. Whatever tool is selected or whatever vendor is contracted with, Centers emphasized the importance of listening to the needs of clinicians and staff and ensuring tools are comprehensive and user-friendly. “Listen to your teams. Every tool is not right for everybody,” Centers advised.
Conclusion and Wrap-Up
During the Q&A at the end of the session on Adoption of AI and BI Solutions, all facilitators emphasized the need for careful application of AI in clinical decision support and the importance of human oversight to ensure accuracy and reliability. “We have to be really, really careful with how we apply extrapolations to things like clinical decision support. I don’t think we’re there yet, and that’s why we’re further along on the business intelligence side,” one of the facilitators noted.
“But you can trust that AI is superior to unaugmented humans when reading anything that requires a pattern…data on MRI, CT, ultrasound, colonography, and PET have all shown that augmented reads of those patterns are more accurate with a computer helping a radiologist,” shared Dr. Flora. “The danger [is] that in 3 or 4 of those studies, when the human overruled the computer, they were often wrong to do so.”
Concerns about AI being used for corporate medical decision-making were also raised. One facilitator stressed the importance of clinician-led AI adoption to ensure that these tools are used to enhance patient care rather than purely for corporate interests. “It’s our responsibility to train our teams, to vet these technologies, and to give the leadership development needed to understand that this is their new world,” he emphasized.


Facilitators
Setting the Stage
Lili Hay opened the session by framing the conversation around the growing pressures cancer programs face. “In health care, we’ve traditionally relied on each other, as well as regulators, payers, and policy makers, to guide our evolution. However, the forces driving our future now extend beyond the health care sector. They stem from a broader realm of technological innovation, reshaping industries at an unprecedented pace and in ways we’ve never before experienced.” She emphasized the need for seamless access, personalized care, and technology-enabled solutions that meet patient expectations. “Patients are expecting more from their health care experiences,” Hay noted, highlighting the importance of adapting to these demands. “Patients are not thinking about regulatory hurdles, workforce shortages, reimbursement models, and all the challenges that we [providers and cancer care programs] live and breathe every day. Patients are just thinking about the care that they need and when and how they need it.”
Pulling from her extensive experience in health care technology, particularly her role as CIO (Chief Information Officer) at Baptist Health South Florida, Mimi Taylor underscored the importance of keeping the patient at the center of technology initiatives. “The patient is the center of our universe, and anything that we do from a technology standpoint has to revolve around that,” Taylor stated.
Taylor went on to share that “implementing technology in health care brings significant accountability, necessitating a practical, thoughtful, and methodical approach.” This approach involves careful selection of the technology, thoughtful implementation planning, and an understanding of how organizational changes will impact everyone involved. Taylor emphasized the importance of supporting new systems and processes, especially after they are introduced, as well as documenting metrics well in advance of starting any implementation work to measure success and ensure the technology effectively addresses the identified problems.
Stephanie Hobbs echoed these insights into strategic planning and operational improvements, agreeing that successful cancer programs employ a structured approach to technology adoption. “Aligning with your health system or overall IT strategies is crucial,” Hobbs advised, reflecting on her experiences as a cancer program administrator.
“Start somewhere, right, and then go from there,” Blackmore suggested. “The more you can solve with 1 partner in this space, the better.”
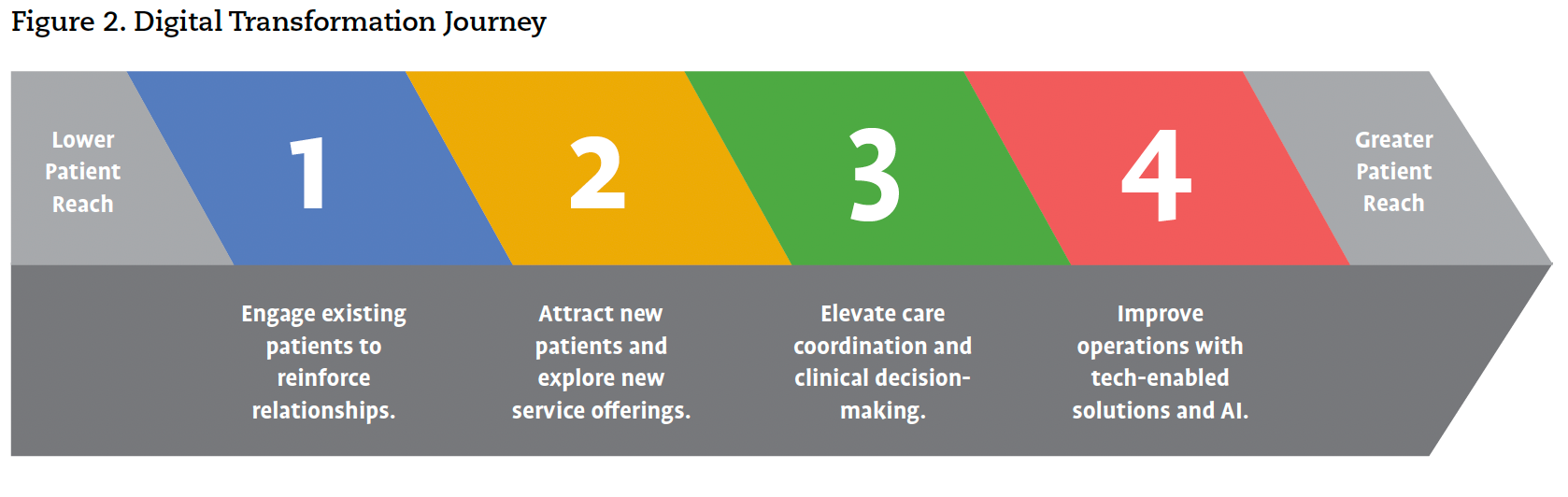
“Digital transformation is a journey that involves leveraging existing investments, optimizing them wherever possible, and wrapping new technology around those investments to enhance patient access, improve operational efficiency, and meet the evolving demands of health care,” Taylor explained. Figure 2 is an illustration of the digital transformation journey.

An Industry Perspective on Technology and AI
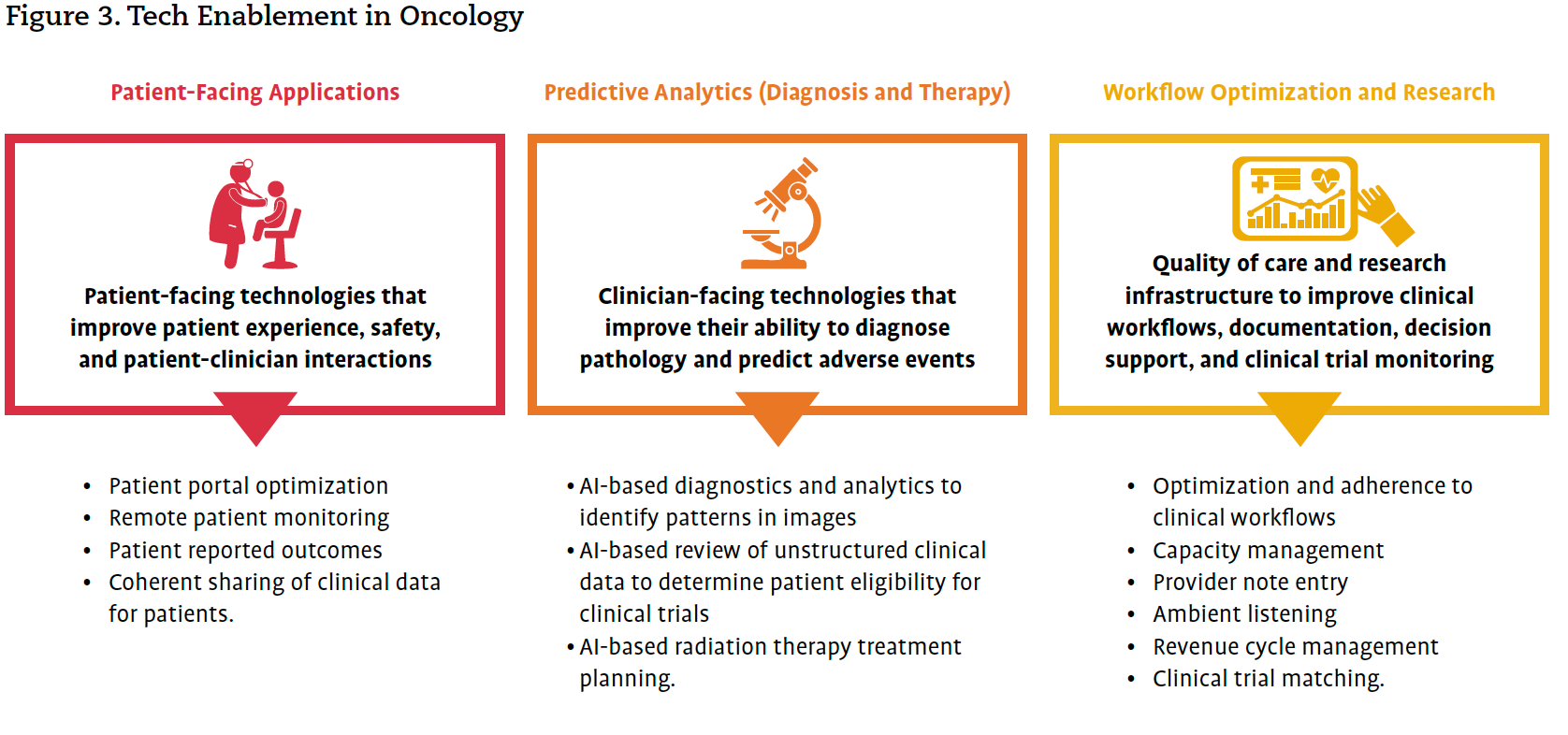
Brooke Blackmore discussed the health care industry’s shift towards AI-driven workflow automation and strategic partnerships, noting that health care organizations are increasingly comfortable trusting AI and other tech-enabled solutions for specific-use cases (Figure 3). Blackmore encouraged attendees to start small and build from there when implementing AI solutions in oncology. She stressed the importance of identifying high manual administrative processes and repetitive tasks and leveraging AI to streamline these processes and tasks, freeing up valuable time for health care professionals to focus on direct patient care.

Blackmore encouraged cancer programs to take incremental steps towards digital transformation, leveraging AI to enhance patient access and care delivery. “Start somewhere, right, and then go from there,” Blackmore suggested. “The more you can solve with 1 partner in this space, the better.” She explained that choosing vendor partners that can address multiple needs over time helps to ensure a comprehensive and scalable solution.
Blackmore provided additional strategies for successful technology implementation, emphasizing the need for a collaborative approach with IT departments from the outset. She recommended creating a playground environment for users to familiarize themselves with the system before going live, allowing users to explore and gather questions at their own pace. By aligning technology initiatives with organizational goals and involving diverse stakeholders, providers can effectively navigate the complexities of technology adoption. Her insights underscore the importance of collaboration, strategic planning, and continuous improvement in the journey towards tech enablement in oncology.
Taylor advised, “Become best friends with your CIO and CFO, so they can learn and live in your world for a little while.”
Hobbs echoed the importance of collaboration and strategic planning in the below use case study on improving infusion throughput. She emphasized the importance of aligning with the CIO and having a well-defined project management plan. “Had I aligned it with the CIO, had I aligned it with a bigger strategy, and really tapped into the resources that were available, implementation would have gone a lot better,” Hobbs reflected.
Use Case Study on Infusion Throughput
Understanding the problem or issue at hand is crucial before considering the adoption of any new technology, including AI. As Taylor explained, “Technology is an enabler; identify problems first and then, if technology can help, organizational readiness is key.” This thoughtful and methodical approach ensures that the technology solution is tailored to address specific challenges. By thoroughly evaluating the problem, organizations can determine the appropriate solution and avoid unnecessary investments in technology that may not meet their needs.
Extrapolating this approach in a use case study, Hobbs first identified a problem: inefficient infusion scheduling, which was affecting patient care and operational efficiency at her former cancer program. To address this problem, Hobbs found a promising solution and began the process of getting it approved and implemented within her health care system.
One of the first hurdles she encountered was the need to align the new technology with existing systems, particularly the health care system’s EHR. “Can’t Epic do that?” was a common question from C-suite leadership, prompting Hobbs to verify Epic’s capabilities and confirm that it could not meet the specific needs of the infusion scheduling solution. While this step delayed implementation, it was crucial in building a compelling case for the new technology.
The next challenge she faced was funding. Securing budget approval for new technology is often a significant hurdle. Hobbs had to get creative with financing options, proposing a monthly expense model to avoid the lengthy capital budget process. By framing the expense as a recurring monthly cost, Hobbs was able to gain approval more quickly and move forward with the next step: implementation.
Once the agreement was signed, Hobbs turned her focus to the implementation phase. “A dedicated project manager and a well-defined project management plan are crucial for successful implementation,” advised Hobbs. “Clear ownership and accountability ensure that everyone knows their roles and responsibilities, which helps cancer programs navigate challenges and achieve the desired outcomes.” This approach not only ensures that everyone knows what is expected of them, but it also allows for clarity in identifying and addressing issues promptly, maintaining project momentum, and avoiding bottlenecks. The project management plan serves as a roadmap, outlining the steps, timelines, and resources required for successful implementation. A structured plan and a dedicated leader to oversee the implementation process are key to success.
During the go-live phase, Hobbs encountered several issues. For example, the reports generated by the new system did not look as expected. More troubling, not all staff embraced the new technology, resulting in only partial usage of the system. These challenges made it clear that the initial training had not been sufficient to ensure a smooth transition, underscoring the importance of ongoing training and support. To address these issues, Hobbs implemented a series of retraining sessions to ensure that all staff members were fully comfortable with the new system. “We did a staggered training during lunch hours and mornings,” Hobbs explained, ensuring minimal disruption to patient care. Additionally, some staff members were sent to the vendor’s home office for more in-depth training. By providing continuous support and opportunities for staff to familiarize themselves with the system, Hobbs improved the accuracy of the reports and increased overall system usage.
In terms of outcomes and impact, implementation of the new infusion scheduling solution led to significant improvements in patient care and operational efficiency. Hobbs reported that the technology facilitated better management of infusion chairs, allowing for more precise scheduling and reducing wait times for patients. These changes improved both provider and patient satisfaction. The new system also helped to improve staffing and workforce efficiency.
Specifically, automation and optimization of the scheduling process reduced the administrative burden on staff—freeing them up to focus on patient-facing tasks—created a more balanced workload, and ultimately reduced provider burnout. Hobbs noted that the enhanced scheduling capabilities also allowed for better utilization of resources, ensuring that staff were allocated effectively based on patient needs. The impact on patient throughput was particularly noteworthy. The streamlined scheduling process enabled the infusion center to accommodate more patients without compromising the quality of care.
Communicating With Strategic Partners and the C-Suite
To build a compelling case for adopting any new technology, all facilitators agreed that it’s crucial to think like the C-suite by understanding the organization’s goals and aligning the proposal with its mission and vision. Taylor advised, “Become best friends with your CIO and CFO, so they can learn and live in your world for a little while.” By presenting a well-documented project management plan with clear metrics and demonstrating how the technology will solve specific problems, the value and necessity of the investment can be effectively communicated to decision-makers. Taylor emphasized the importance of collaboration and strategic partnerships. By fostering strategic partnerships, health care organizations can leverage the expertise and resources of their partners to develop and implement effective technology solutions. This collaborative approach ensures that the technology is aligned with the organization’s goals and can address specific issues in cancer care, such as patient access, treatment coordination, and operational efficiency. She advised that cancer programs should not work in isolation but rather engage with various stakeholders, including administrators, clinicians, IT departments, and vendor partners, to ensure a comprehensive approach. “Collaborate as a strategic partner and develop a cancer-specific plan,” Taylor recommended.
A Framework for Success
The session concluded with a discussion on organizational readiness and the importance of a structured framework for evaluation and implementation of technology solutions. Taylor emphasized that technology alone is not the solution; it requires a comprehensive approach that includes C-suite support, technical infrastructure, funding, talent, and timing. This structured framework ensures that organizations are prepared to adopt new technologies effectively and sustainably.
As discussed above, the framework begins with a thorough understanding of the problem or issue that needs to be addressed. Organizations must define the problem clearly and assess whether technology is the appropriate solution. This involves evaluating the integration complexity, considering alternative approaches, and assessing organizational readiness. Taylor highlighted the importance of documenting metrics well in advance to measure the success of the implementation.
Next, the framework includes collaboration with the diverse stakeholders identified earlier to develop a comprehensive plan. Clear ownership and accountability are crucial to help navigate unanticipated challenges and achieve the desired outcomes.
The framework also emphasizes the need for ongoing training and opportunities for staff to familiarize themselves with the new technology. Strategies discussed previously include staggered training sessions, refresher courses, and a playground environment for users to explore the system before it goes live.
Taylor emphasized that technology alone is not the solution; it requires a comprehensive approach that includes C-suite support, technical infrastructure, funding, talent, and timing.
Finally, the framework includes a strategic approach to gaining C-suite approval, aligning technology initiatives with organizational goals and involving diverse stakeholders. As cancer care continues to evolve, the adoption of technology-enabled solutions will be crucial in addressing patient access issues and improving overall care delivery. The insights and experiences shared here provide a valuable roadmap for organizations looking to navigate the complexities of tech enablement in cancer care.


Facilitators
Virtual APP Visits Increase Revenue and Improve Patient Access and the Patient Experience
Calliope Bodenhorn Payne shared how adoption of virtual advanced practice provider (APP) visits helped Texas Oncology expand its service lines and grow the organization, retain more patients and attract new patients, and improve provider well-being by offering flexibility in scheduling and reducing burnout. For cancer centers and practices that might want to develop a similar program, she shared how the program was designed, implemented, and continuously improved.
Program Design
The inception of Texas Oncology’s Virtual Care Program was driven by the urgent need to provide oncology care during the COVID-19 pandemic. “How do doctors treat their cancer patients when it’s unsafe for that population to even leave their homes?” Bodenhorn Payne asked. The solution was to rapidly ramp up telemedicine services. To do so, Texas Oncology formed a dedicated team to cover the spectrum of patient needs, from remote triage nurses to telemedicine support staff and fully remote APPs.
By the end of 2021, the Virtual Care Program was staffed by a team of 4 highly experienced APPs, each with distinct skill sets. These providers signed collaborative agreements with Texas Oncology’s medical director and were given standardized training and credentialing.
“Our APPs were also provided with extensive resources and support, such as site contact information, patient community resources, and standardized workflows and order sets,” Bodenhorn Payne explained. This comprehensive preparation meant APPs could support multiple Texas Oncology sites statewide. “Leadership determined which diagnoses are appropriate to be seen by the APPs and which are not,” Bodenhorn Payne clarified, ensuring that the program addressed the most pressing patient and provider needs.
For Texas Oncology, the addition of benign hematology services to the patients seen by the APP team was a strategic move to address patient dissatisfaction.
Program Implementation
The implementation phase began with APPs supporting 12 Texas Oncology sites and covering various appointment types, including genetics, advanced care planning, treatment review, and urgent care. Within 3 months, these APPs had seen more than 100 patients. The impact on patient access was staggering. “Patients went from being told they would have to wait weeks to be seen to being able to speak with a provider in a matter of days,” Bodenhorn Payne shared.
As the program expanded, additional APPs were hired, and the team grew to 8 full-time APPs and 1 part-time APP. The Virtual Care Program also added more telemedicine support staff, including schedulers, patient service coordinators, medical assistants, and a patient benefit representative. This expansion allowed the APP team to target new areas of need, such as benign hematology diagnoses, which previously had longer wait times.
For Texas Oncology, the addition of benign hematology services to the patients seen by the APP team was a strategic move to address patient dissatisfaction. Benefits were 2-fold: expansion allowed the APPs to practice at the top of their licenses and significantly reduced wait times for benign hematology patients. “These patients were able to get appointments approximately 21 days earlier than if they had had to wait for an opening in the clinic,” Bodenhorn Payne said. Timely access to care helped alleviate patient frustration and dissatisfaction, ensuring that patients received the necessary medical attention without prolonged delays.
Provider Benefits
The Virtual Care Program provided numerous benefits to Texas Oncology providers, enhancing their work-life balance, reducing burnout, and improving overall job satisfaction. One of the most significant advantages was the flexibility in scheduling, which allowed providers to take well-deserved time off without disruption of patient care. “Whether the provider needs a week-long vacation or a 12-week maternity leave, the patients who had been on the schedule to see those providers can easily be transitioned to virtual APP appointments,” Bodenhorn Payne explained. This flexibility ensured that patient appointments were not canceled or rescheduled, maintaining continuity of care and reducing stress for both providers and patients.
The Virtual Care Program also helped alleviate the workload for clinic providers, with APPs taking on time-consuming appointments, such as 40- to 60-minute chemo teaches and survivorship classes. “[In-person] clinics were freed up to take on more of those shorter appointment times, theoretically being able to see anywhere between 2 to 4 patients for each one of those 60-minute time slots,” Bodenhorn Payne explained. This workload redistribution allowed clinic providers to focus on more acute cases, improving efficiency and productivity.
Finally, as mentioned above, the Virtual Care Program allowed APPs to work at the top of their licenses on treatment plans, symptom management, and genetic risk assessment. This level of care not only benefited patients but also improved the professional satisfaction of the APPs. “We don’t have the distractions that come with working in a busy clinic and are able to focus more directly on the patient,” Bodenhorn Payne noted. This ability to provide unhurried, one-on-one consultations contributed to a sense of ownership and fulfillment in their roles.
The positive impact on provider turnover and burnout was evident. “Our providers do seem pleased with the freedom and flexibility of scheduling, with internal studies showing a decrease in provider turnover and burnout,” Bodenhorn Payne reported. The Virtual Care Program’s success in retaining staff was further underscored by the 0% turnover rate among virtual APPs in the last 3 years, highlighting the program’s effectiveness in maintaining a satisfied and stable workforce.
The Virtual Care Program’s impact on operational efficiency has been profound. Tangible benefits to Texas Oncology included increased appointment availability, higher patient satisfaction, and improved revenue. As mentioned above, by taking on time-consuming appointments, the virtual APPs freed up clinic providers to see more patients with acute needs. This led to a significant increase in patient throughput and revenue. Additionally, the virtual care team streamlined processes, such as ensuring labs had the necessary genetic testing kits and simplifying order sets, which reduced out-of-pocket costs for patients and the rate of insurance denials. The program’s success is reflected in the numbers: a 138% increase in referral volume since its inception, with virtual APPs now supporting about 1000 patient appointments per month. This increase in patient volumes naturally generated significantly more revenue for Texas Oncology. The reduction in no-show and cancellation rates further underscores the program’s effectiveness. “Our APPs have fewer patients canceling their appointments or not showing up for their calls,” Bodenhorn Payne reported, attributing this to the convenience and attention provided through telemedicine.
Patient Benefits
On the patient side, benefits included timely access to care, financial savings, and the convenience of telemedicine, which minimized disruptions to their daily lives and increased patient satisfaction with care. The process of connecting with a virtual patient service coordinator, medical assistant, and APP took about 8 minutes in total. “Patients went from having to wait 18 minutes—from the time they began the call to being connected to an intake specialist or provider—to having to wait less than 2 minutes to be connected with a virtual patient coordinator,” Bodenhorn Payne explained. This streamlined process not only saved time but also reduced the stress and frustration associated with long wait times.
With the Virtual Care Program, patients were able to receive care from the comfort and safety of their homes, eliminating the need for travel and reducing the time spent away from work or other obligations. An internal study conducted by the virtual care team at Texas Oncology revealed that patients typically missed approximately 3.5 hours of work per appointment due to commute and visit time. With virtual APP visits, this burden was significantly reduced, allowing patients to maintain their daily routines with minimal interruption.
“We want to reduce the number of repeat testing and the patient travel to repetitive appointments,” LaRaia emphasized.
In addition to enhanced convenience and time savings, the Virtual Care Program also saved patients money. The same study concluded that the average patient missed out on just under $100 of pay per appointment, plus the additional expense of commuting, which was a little less than $10 per trip. By eliminating the need for travel, virtual APP visits helped patients save on transportation costs and avoid lost wages, which could make a substantial difference in their weekly budgets. “Honestly, that’s a sum that could make or break a weekly budget for a lot of our patients who really have enough to be worried about without also having to be concerned about finances when a solution to that is readily available,” Bodenhorn Payne noted.
The virtual APPs have also played a crucial role in improving preventative health, providing genetic risk information, and keeping acute patients out of the ED with same-day urgent care appointments. Efforts to bridge the accessibility gap continue, with Texas Oncology’s Virtual Care Program providing additional services like navigation and palliative care. As Bodenhorn Payne concluded, “APPs are setting a new standard for oncology care at Texas Oncology,” demonstrating the transformative potential of virtual care for other cancer programs looking to replicate this care model.
A Rapid-Access Oncology Diagnostic Clinic Increases Referrals and Reduces Time to Treatment
Inspired by a 2022 ACCC Innovator Award presented to The Ohio State University Comprehensive Cancer Center – The James, Kathleen LaRaia shared Munson Healthcare’s experience of adapting this innovation to implement a rapid-access oncology diagnostic clinic to meet the unique needs of its rural Michigan community.
Program Design and Implementation
Munson Healthcare and its Cowell Family Cancer Center operate under a hub-and-spoke model, with medical oncologists attending outreach sites weekly. LaRaia highlighted the significant barriers to oncology care in rural areas, including incomplete diagnostic workups and a shortage of primary care providers (PCPs). “Ninety percent of our patients with cancer were presenting to the ED for the first time,” she noted, emphasizing the urgency of addressing these challenges.
To overcome these obstacles and stand up the rapid-access oncology diagnostic clinic, LaRaia enlisted the support of a physician champion, who agreed to serve as the collaborative provider for 2 APPs from existing staff. The program would focus on patients presenting with new abnormalities on imaging, typically in the ED, and aimed to expedite their diagnostic workup and referral to oncology care.
Implementation required a multifaceted approach, which required extensive communication and education efforts. “I needed a dramatic shift in provider culture to convince them to see patients who had an incomplete workup,” LaRaia explained.
Financial considerations also played a huge role, specifically billing and coding for initial consults. LaRaia noted, “If an APP saw that patient, then the physician didn’t get the first initial consult. E/M [evaluation and management] codes and RVUs [relative work value units, standardized measures used to quantify the resources required to provide various medical services] are still an issue today.” When APPs bill for services under their own national provider identifier (NPI), they are reimbursed at only 85% of what physicians are paid.
Because many of the hospitals within the health care system were on different EHRs, Munson Healthcare initially piloted the oncology diagnostic clinic with hospital EDs that were on the Cerner system, as it allowed the cancer center to create a referral button within the EHR. Data from the 6-month pilot found:
The rapid-access oncology diagnostic clinic was rolled out without additional FTEs, relying instead on collaborative efforts among existing staff. LaRaia recruited passionate individuals from specialty clinics, including the multidisciplinary thoracic oncology team, the palliative care clinic, and the bleeding disorders clinic. Initially, the process did not involve virtual visits; APPs reviewed referrals, contacted patients, and determined next steps for diagnostic tests. Based on feedback and challenges encountered in this process, “we learned that we needed to advance this [program] to include virtual visits and telehealth visits,” shared LaRaia.
When clinic expanded to other hospitals, the cancer center created additional referral mechanisms, including a direct fax number and a phone number for intake specialists. To ensure referrals were processed efficiently, “we needed to create referral redundancy because many of the hospitals were on disparate EHRs,” LaRaia explained.
Since the expansion, the rapid-access oncology diagnostic clinic has had 415 referrals to date, and is now being rolled out to hospitalist groups and PCP (primary care provider) practices. To secure additional resources—including FTEs—the program is tracking metrics such as time from suspicion to treatment, repeat testing, and patient travel.
Patient and Provider Benefits
The rapid-access oncology diagnostic clinic has yielded significant benefits for both patients and providers. “Our oncologists can tell which patients have come through the diagnostic clinic because they’re much more relaxed,” she said. Patients appreciate the streamlined process, which reduces anxiety and ensures timely access to care.
ED providers and hospitalists have expressed tremendous satisfaction with the program. LaRaia shared the relief these providers feel knowing patients are connected to the cancer center. The program has also decreased inpatient length of stay, allowing hospitalists to focus on other patients. “Inpatient hospitalists had wondered why certain patients were staying in a bed waiting for pathology results when they [could] go home,” she clarified.
The program has created better collaboration between oncology and primary care. Michigan’s busy PCPs appreciate the streamlined referral process that allows them to quickly connect patients with oncology specialists. This improved collaboration reduces the burden on PCPs and ensures that their patients receive timely and appropriate care.
Additionally, the rapid-access oncology diagnostic clinic has led to increased efficiencies in radiology and laboratory procedures. LaRaia, who also oversees radiology and lab services, reported growth in both areas. This growth reflects the program’s success in optimizing diagnostic processes.
For patients, the rapid-access oncology diagnostic clinic has significantly reduced the time from initial suspicion of cancer to treatment. This expedited process is crucial in oncology, where timely intervention can greatly impact outcomes. As mentioned above, patients who come through the clinic are better prepared and less anxious, having already interacted with the health care team and undergone necessary preliminary tests.
The rapid-access oncology diagnostic clinic also addresses the issue of repeat testing and unnecessary travel for patients. By ensuring the right diagnostic workup is done the first time, patients avoid the frustration and inconvenience of multiple appointments and tests. “We want to reduce the number of repeat testing and the patient travel to repetitive appointments,” LaRaia emphasized. This approach not only improves patient satisfaction but also improves the overall efficiency of the health care system.
Interactive Q&A
Following LaRaia’s presentation, attendees engaged actively, sharing their experiences, posing insightful questions, and providing valuable lessons and learned.
One attendee, who works in a large health care system, shared efforts to incorporate a similar process and emphasized the importance of a catchy term for the clinic. “We’re still in the midst of figuring out what kind of adjustments we need to make,” this attendee acknowledged. “One of the things we have been able to incorporate is physician education about billing and coding.” This feedback reinforced the need for clear communication and education to ensure provider buy-in and appropriate compensation.
Another attendee from Penn Medicine in Philadelphia highlighted the role of oncology nurse navigation in clinical triage. They shared how nurse navigators helped direct patients to the appropriate diagnostic tests and specialists, reducing delays and improving patient outcomes. “We really harnessed oncology nurse navigation to do a lot of clinical triage via the phone, looking at medical records, and we didn’t always send patients directly to medical oncology,” the attendee explained.
Munson Healthcare’s rapid-access oncology diagnostic clinic has transformed oncology care in Northern Michigan and for the rural patient population it serves.
A question from the audience focused on service-level agreements with radiology for specific turnaround times on imaging and workups. LaRaia responded that their “radiology group is already robust. They’ve been able to recruit, and so their turnaround time has always been 24 hours.” This exchange highlighted the importance of having reliable and timely diagnostic services to support rapid access clinics.
Another question addressed the appropriateness of referrals and the potential for overwhelming the clinic with unnecessary cases. LaRaia explained that Munson Healthcare had largely avoided this scenario because APPs had been given comprehensive education and guidance from the physician champion.
An audience member from a health care system undergoing a merger shared their experience with an “undiagnosed mass clinic” that quickly became overwhelmed with referrals. This feedback highlighted the need for scalable solutions and continuous monitoring to prevent burnout and maintain quality care.
Munson Healthcare’s rapid-access oncology diagnostic clinic has transformed oncology care in Northern Michigan and for the rural patient population it serves. As cancer centers across the country continue to adopt value-based care strategies, development and implementation of similar programs will be crucial. By addressing barriers to care, optimizing diagnostic processes, and fostering interdisciplinary collaboration, these cancer centers can pave the way for a more efficient, effective, and patient-centered oncology care delivery system.
Development of a Virtual Cancer Center
It all started when Kaiser Permanente, an integrated health care model serving 12.4 million members across 10 states with 67 oncology clinics, wanted to implement a standardized approach to ensure consistent, high-quality care for all patients, regardless of where they lived. But why is standardization so important, and “How do you bring together 67 clinics sprinkled across the United States that have functioned independently for the last 75 years?” asked Dr. Tatjana Kolevska.
The why was tied to the dramatic increase in the rate at which medical knowledge doubles. In the 1950s, it took about 30 years for medical knowledge to double, said Dr. Kolevska. Flash forward to the 1970s and 1980s, and the time it took medical knowledge to double had decreased to 10 years. “Why do providers need to take the boards every 10 years? Because the doubling time was 10 years,” said Dr. Kolevska. Today, that doubling time is just 3 months. “Is there a human being who can learn all oncology or all medicine every 3 months? Absolutely not.” Instead, today’s providers must look to technology to help them keep pace with the rapid expansion of medical education and information.
Another important piece of the why: the knowledge that “in about 30% of cancer patients, if an expert reviews the treatment, the treatment would be changed,” said Dr. Kolevska.
To address these challenges, Kaiser Permanente leveraged technology to create the how: a Virtual Cancer Center with expert reviews and virtual consultations. These technology solutions enable providers to access up-to-date, evidence-based recommendations and collaborate with specialists across the country. “We use technology to automatically pick complex cancer cases...reviewed by the experts before they’re seen by the frontline oncologists,” Dr. Kolevska explained.
Virtual Cancer Center Design
Dr. Kolevska described how the COVID-19 pandemic served as a catalyst for the rapid creation and implementation of Kaiser Permanente’s Virtual Cancer Center. Prior to the pandemic, only about 15% of Kaiser Permanente’s oncology care was delivered through virtual visits, despite efforts to increase this percentage. “Our leadership met in January 2020, and I was trying very hard to persuade everybody that we should try to aim for 30% that year,” and she was getting pushback, Dr. Kolevska recalled. However, the onset of COVID-19 necessitated a dramatic shift in health care delivery to minimize foot traffic in clinics. “In 1 week, we went from 15% to 98% virtual care [appointments],” Dr. Kolevska recounted. This rapid transition was made possible through patient education and the use of navigators to guide patients in the use of telehealth services. “We had a clinic where all 4 oncologists got sick. We asked patients, ‘Would you like to travel to see somebody or would you like to see somebody virtually?’ All of them chose virtual visits,” said Dr. Kolevska. “So, these opportunities are very real, and that’s what took us to the next level.”
Kaiser Permanente’s Virtual Cancer Center was designed with 2 main wings: the support wing and the expert wing. The support wing focuses on nonclinical care, providing essential services such as financial navigation, social support, and mental health resources. This wing is staffed by trained specialists who assist patients with various nonmedical needs, ensuring patients receive comprehensive support throughout their cancer journey. “We partnered with the American Cancer Society to have its navigation training,” Dr. Kolevska noted, emphasizing the importance of well-trained staff in delivering these services. “We don’t tell patients, ‘You can’t afford your medication. Call AstraZeneca and see if they can help you.’ We actually do it ourselves. We call for patients and we see it through to the end.” And that level of service requires time. “It takes about 30 to 40 minutes when a patient calls and needs help.”
The expert wing comprises 11 specialized departments, including breast cancer, sarcoma, and lung cancer, each staffed by expert teams. These departments provide cutting-edge clinical care and consultations, leveraging the expertise of top oncologists across the country. “We put together our expert teams to support the virtual Cancer Center,” Dr. Kolevska explained. The expert wing offers several key services:
Patient and Provider Benefits
The Virtual Cancer Center has significantly improved access to expert care, regardless of geographic location. Dr. Kolevska shared that more than 50% of patients now choose virtual care, even for consultations. “Right now, I do have patients that I’ve never seen in person,” she said, highlighting the convenience and accessibility of telehealth.
For providers, the Virtual Cancer Center offers a streamlined process for expert consultations. Oncologists can request an expert review by simply entering an order in the EHR. “Instead of typing chest X-ray in order entry, they actually type expert review,” Dr. Kolevska explained. This order is then reviewed by a national coordinator who assigns it to the appropriate expert, ensuring timely and accurate recommendations. “The expert is able to go in the patient chart, review the full chart, the scans, the radiology, and everything that is inside,” explained Dr. Kolevska. “This is not a summary created by a staff member. This is a full chart review…the expert leaves a note in the chart within 2 business days. So that’s how the whole system works.”
The program has also improved equity in cancer care. “The demographics of patients who actually received this service mimicked exactly the demographics of the communities we served,” Dr. Kolevska noted. This ensures that all patients, regardless of age, socioeconomic status, or location, receive the same high-quality care.
Finally, the Virtual Cancer Center has streamlined the referral process, making it easier for frontline teams to access expert opinions. “The best thing to do should be the easiest thing to do,” Dr. Kolevska stated. This simplified referral process has led to high satisfaction rates among oncologists and patients.
Quality Improvement Outcomes
The Virtual Cancer Center has demonstrated significant improvements in care quality and outcomes. Dr. Kolevska shared that the expert review process has led to changes in treatment for approximately 30% of patients. “We just published our data in the New England Journal of Medicine, Catalyst...and guess what? How many doctors said that they changed the treatment because of the expert review? Just around 30%,” she reported.1
The program has also reduced unnecessary treatments and improved diagnostic accuracy. “We decreased the number of patients that receive chemotherapy by half,” Dr. Kolevska stated, referencing a Kaiser Permanente study on testicular cancer.2 This reduction is attributed to the expert review process, which ensures that patients receive the most appropriate, evidence-based care. To explain how this service is reducing health care costs and improving care utilization, Dr. Kolevska shared, “[As a clinician] I will always err on the on the side of doing more. I’m going to give adjuvant chemotherapy because what if the cancer comes back later?…So it’s very interesting that when experts review the care, it usually means giving more concise, up-to-date, cutting-edge care—nothing more, nothing less.”
Lessons Learned and Future Directions
Audience questions and shared experiences during Dr. Kolevska’s presentation provided valuable insights. One attendee asked about the billing process for expert opinions provided through the Virtual Cancer Center: “Is the expert opinion that you are doing, say, from Hawaii to LA, a billable service? Is that something that you’re billing under the patient’s insurance?” Dr. Kolevska explained that while the integrated health plan currently finances this service, the infrastructure for billing was established from the beginning to ensure long-term sustainability. “I heard several times during today’s presentation: How do you persuade physicians and staff that you should move in that direction? And we decided that the best way to persuade them [physicians, staff, and even patients] is to let them try these services,” clarified Dr. Kolevska. While Kaiser Permanente decided to finance the Virtual Cancer Center for the first 3 years, the health system created the technology and the process to be able to bill in the future for these services.
While Kaiser Permanente decided to finance the Virtual Cancer Center for the first 3 years, the health system created the technology and the process to be able to bill in the future for these services.
An attendee from Jefferson Health in Philadelphia asked how providers who are spread across the country are able to see patients from other states. Dr. Kolevska explained that the expert consults are considered curbside consultations, which do not require licensing or credentialing in most states. However, she clarified that Kaiser Permanente is licensing all its expert physicians in the states in which they do second opinions and complex case reviews.
Another attendee raised concerns about the shift toward telehealth and its impact on traditional methods of patient examination. They asked how Kaiser Permanente addresses the challenges of telehealth, especially in terms of inspection and palpation. Dr. Kolevska responded by describing the development of a curriculum for video visit exams, “We realized that a video visit can examine more than 80% of the things we examine in person, if you are very intentional,” she explained. This curriculum is considered in educational settings such as Kaiser Permanente’s residency programs, fellowships, and medical school, preparing providers for the future of telehealth.
Finally, an audience member asked about the future of telehealth and its impact on the Virtual Cancer Center model. Dr. Kolevska emphasized the importance of teaching both the medical community and patients about the possibilities of telehealth. She shared a story about nurse navigators transitioning back to in-person visits after COVID, which led to patients preferring in-person consultations. “To move forward, we must not only educate the medical community about the possibilities, but also educate the patients. Teach patients that they have a choice in how and where they receive their care,” she concluded.
Leveraging Infusion Pharmacy Strategies to Deliver Organizational Value
At the start of his presentation, Jorge García underscored the importance of understanding the market and analyzing the competition. “In my market, in South Florida, when I think about competitors, what immediately comes to mind are other health systems or other providers,” he said. However, he noted that health care disruptors and payers (health care plans) are increasingly providing direct services, which also impacts market share. Use of a payer-owned pharmacy or a specialty pharmacy contracted by a payer “diverts a big portion of the market share that we [cancer programs] could otherwise capture. Because we have the resources, the means, and the drug on our shelf that we could make available to patients right away,” García described. “So that’s an example of how we may be competing directly with our health plans.” He then went on to outline Baptist Health Pharmacy’s strategic approach to expanding infusion services, increasing revenue, and meeting patient demand.
In addition to cost savings through reduced LOS and bed capacity optimization, Baptist Health Infusion Care has opened up new revenue streams for the health care system.
Ensuring Revenue Integrity
Revenue integrity involves ensuring that the health care organization accurately captures and maximizes revenue for the services provided through meticulous auditing, analysis, and monitoring of payer claims. At Baptist Health South Florida, pharmacy revenue integrity includes management and oversight of new drug onboarding, the charge master, performance dashboards for activities like biosimilar use and infusion center performance, claims denials, and pharmacy business modeling and pro formas.
Effective charge master management requires an understanding of drug costs. García described the process of auditing payer claims to understand payment specifics at the J-code level (billing codes used for injectable drugs). “We have retrospectively, many times and in more manual ways than I would have liked, gone back to payer claims, drug by drug, patient by patient, to identify specifically how much we got paid for that J-code,” he explained. This detailed analysis allowed Baptist Health to understand the exact payments received for each drug and then develop a charge master strategy that ensured consistent and reasonable pricing. This strategy involved grouping drugs by cost and adjusting markups. For example, higher markups were applied to complex therapies like carboplatin, while lower markups were applied to high-cost immunotherapies to ensure affordability.
Revenue integrity also involved creating dashboards specific to biosimilars and other drug categories, allowing the organization to monitor and optimize its formulary. This approach helped Baptist Health align inpatient and outpatient drug types, optimize 340B resources, and diversify its service mix, ultimately leading to new revenue streams.
While “neutral cost shift,” which refers to the idea of redistributing costs within a health care system in a way that does not increase overall expenses but reallocates them from one area to another, is a strategy often proposed by payers during negotiations, García urged caution. “In the short term, that approach may be neutral. However, when you think long term, and you look at how imaging services are expected to expand over the years, and you look at your drug pipeline and how that is expected to expand over the years, what would be a neutral shift of cost today could have great impact on the charges and the reimbursement you get in the future,” he explained. In other words, as demand for imaging services grows and the drug pipeline expands, this shift could lead to significant changes in reimbursement and financial sustainability.
Growing Ambulatory Infusion
García received weekly calls from providers with questions about administering drugs when they lacked infusion capabilities and whether to send patients to the ED or hospitalize them for administration, which was costly and not ideal for patient care. Additionally, Baptist Health was seeing patients travel across county lines, seeking infusion providers for their medication. Recognizing this growing demand for infusion services, García and his team conducted research to understand patient needs and forecast future trends. “It was quickly realized...that there was an expansive pipeline of products coming in IV dosage form,” he said. This led to the development of a comprehensive strategy to expand infusion capabilities across Baptist Health’s facilities and the creation of Baptist Health Infusion Care.
Today, Baptist Health Infusion Care encompasses both oncology and nononcology infusion capabilities, with a focus on expanding access and improving patient care across the 4 southernmost counties of Florida. Infusion services are hospital-based, providing access to 340B drug pricing and leveraging existing hospital contracts. This structure allows Baptist Health Infusion Care to offer comprehensive infusion services, including high-cost and specialized medications, while maintaining a focus on revenue integrity and patient-centered care. The infusion centers also support hospital operations by reducing inpatient stays and facilitating outpatient care, thereby optimizing resources and improving patient outcomes.
Creation of Baptist Health Infusion Care was not without its challenges:
Understanding 505(b)(2) Medications
After an informal poll showed that only 1 attendee was familiar with the 505(b)(2) FDA approval pathway, García outlined its potential benefits. He explained that this pathway allows for expedited approval of molecules that have already been thoroughly tested. These are small molecules—not biologics or biosimilars—and include drugs like carboplatin and cyclophosphamide. The pathway enables formulation enhancements, such as eliminating the need for reconstitution in IV rooms or reducing labor expenses associated with sterile supplies. These drugs can then come to the marketplace with a higher price, offering cancer programs better cost recovery on these products.
García noted that the 505(b)(2) pathway could also help address drug shortages, as it provides a viable and sustainable way to bring essential drugs to market. He highlighted concerns about the sustainability of sterile products that cost less than a cup of coffee, emphasizing the need for more viable options moving forward. García urged attendees to explore how the 505(b)(2) pathway could fit into their practices, as it offers hope for maintaining the backbone of cancer care in a more sustainable manner.
Operational Benefits
García explained that Baptist Health Infusion Care has significantly reduced hospital length of stay (LOS). Many patients who require IV drug therapy can now be discharged from the hospital and complete their treatment at 1 of the 10 outpatient infusion centers. This approach allows patients to receive the last few days of their IV therapy in a more convenient and less costly outpatient setting, rather than occupying a hospital bed. García noted that this strategy has added substantial value, especially at their flagship hospital, which frequently operates at full capacity. By transitioning patients to outpatient infusion centers, Baptist Health can free up hospital beds for other patients in need of acute care. This not only improves patient flow and reduces bottlenecks in the ED but also enhances overall hospital operations and patient outcomes. In addition to helping during “code black days when there are more patients waiting in the ED to be admitted than we have available beds,” García said the 10 Baptist Health Infusion Care locations help “reduce the ‘noble effect’ where patients are waiting in sister facilities for services only offered at the main hospital” by managing patient transitions and optimizing hospital resources.
In addition to cost savings through reduced LOS and bed capacity optimization, Baptist Health Infusion Care has opened up new revenue streams for the health care system. García explained that expansion into areas outside of oncology, such as hematology and rare disease pharmaceuticals, allows Baptist Health to meet the varied needs of its patient population and provides growth opportunities in different therapeutic areas. “Our infusion centers don’t just have to be an infusion center. They could be anemia clinics,” he noted with an eye to the future. By hiring specialized staff, such as a doctoral-prepared pharmacist with expertise in neurology, García highlighted the potential of offering specialized neurology services within the outpatient infusion center setting.
García ended with a call for his colleagues in the room to take action and explore how these strategies can be implemented in their own cancer programs. Invest in infrastructure, educate stakeholders, and leverage existing resources to meet the growing infusion needs of your patient population, he advised. By doing so, you can improve patient access and outcomes, streamline processes, and help ensure the financial sustainability of your cancer program.

Facilitators
Tynan Kugler kicked off the 2-hour deep dive by sharing the session objectives: to understand national oncology trends, to explore why cancer programs pursue partnerships and affiliations, and to discuss the implementation and sustainability of these collaborations.
National Oncology Partnership Trends
Facilitators identified these trends as drivers of oncology partnerships and affiliations:
Partnership Structures
The panel discussed several possible partner structures, each with unique benefits and considerations:
Why Cancer Programs Pursue Partnerships and Affiliations
To increase clinical trial access. By collaborating with academic centers and larger health systems, community cancer programs get access to a broader range of clinical trials, increasing treatment options for patients that might otherwise be unavailable to them. Serig said that “Clinical trials [are] always the number 1 thing that we want to bring to the table” in any partnership or affiliation.
To expand access to programs and services. Beyond research, partnerships and affiliations also allow community cancer programs increased access to specialized care and advanced treatments. Serig shared that her health care system’s experience of offering navigation services to a program that previously lacked access to such services was transformative. By providing these essential services, the community cancer program was able to streamline the treatment process and help ensure that patients received timely and coordinated support. Scott emphasized this benefit, stating, “Our goal is to make the community program stronger in its cancer care.”
To provide higher-quality cancer care. Partnerships and affiliations allow cancer programs to implement quality improvement measures and improve patient care through shared best practices and collaborative efforts. Fernandez emphasized the importance of quality improvement, stating, “Once we level set that partnership, then the question becomes, How do we start infusing data, quality, and performance improvement to elevate services across the entire network?” Fernandez emphasized that community and academic programs are equal partners in these collaborations, with both parties bringing valuable insights and practices to share. She noted that these partnerships are mutually beneficial, with community programs often adopting best practices from academic centers, while academic centers also learn and integrate effective strategies from their community counterparts. This reciprocal relationship fosters a collaborative environment where both parties grow and improve together.
To maximize treatment capacity. Successful affiliations and partnerships can improve operational efficiency and optimize treatment capacity by enabling the sharing of resources and facilities between the collaborating entities. For example, community cancer programs may have available infusion treatment chairs, MRI slots, or linear accelerator time that can be utilized by partnering institutions facing capacity constraints or vice versa. By sharing resources, partner organizations can also reduce wait times for patients, which is particularly critical in oncology, where timely access to treatments can significantly impact patient outcomes. Serig emphasized this benefit, noting, “It is an opportunity to partner with community hospitals and cancer centers who have capacity to share with us.”
To increase market reach or market share. Scott discussed how affiliation with Dana-Farber Cancer Institute significantly helped her community cancer program increase its market share. By partnering with Dana-Farber, her program leveraged the brand’s reputation and expertise, attracting more patients seeking high-quality cancer care. This collaboration not only enhanced the community cancer program’s credibility but also provided access to specialized treatments and clinical trials, further boosting patient enrollment and expanding the program’s reach. Affiliations and partnerships can also extend the geographic reach of cancer programs by establishing satellite clinics or collaborative networks in underserved areas, essentially growing the cancer program’s market presence.
To support recruitment efforts. Affiliations with academic centers and larger health care systems provide access to a broader network of health care professionals, including oncologists, APPs, nurses, and support staff like navigators, social workers, and dietitians. This expanded talent pool can help community hospitals recruit highly qualified candidates. Scott mentioned that her program’s affiliation with Dana-Farber Cancer Institute provided valuable support for physician recruitment, noting, “Dana-Farber will help with recruitment; that is part of our contract.” Partnerships often include opportunities for training and professional development, which are attractive to potential recruits. Access to specialized training programs, fellowships, and mentorship from renowned institutions can be a significant draw for cancer care professionals. Finally, affiliations and partnerships can provide financial incentives and stability; access to funding for research, competitive salaries, and benefits are all important to potential recruits.
To grow programs and services. Successful affiliations and partnerships support strategic planning efforts. “We do offer strategic planning so that we can bring our expertise with SWOT [Strengths, Weaknesses, Opportunities, Threats] analysis,” shared Fernandez. Working in collaboration, SWOTs can help both partners identify internal and external factors that can impact their success. Moreover, affiliations bring together diverse perspectives, enabling a comprehensive SWOT analysis that considers various viewpoints and expertise. Pulling the SWOT through to strategic planning allows the partnering organizations to identify gaps in existing services and opportunities for growth. For example, a community hospital might lack certain specialized services that an academic center can provide. By recognizing these gaps, the partnership can develop programs or processes to address them.
“Access to clinical trials is a key element because it allows cancer programs to offer cutting-edge treatments to patients locally, increasing their care options and potentially improving outcomes,” said Serig.
What Cancer Programs Look for in a Partner
The Implementation Process
Successful partnerships and affiliations generally follow these steps:
Key Takeaways
Scott emphasized the importance of internal marketing to departments and service lines before publicizing the affiliation to ensure that the staff and internal stakeholders fully understand and appreciate the benefits of the partnership. This approach helps build trust and credibility within the organization, making the transition smoother and more effective. By focusing on internal marketing first, the cancer program can address any concerns or misconceptions among the staff, ensuring that they are well-informed and supportive of the affiliation. This internal buy-in is crucial for the successful implementation and promotion of the partnership to the broader community.
Serig stressed the importance of being present and fostering ongoing communication. “These relationships take presence that is ongoing and a concerted effort,” she noted. She described the importance of transparency and visibility, ensuring that both parties are aligned in their goals and decision-making processes.
Fernandez shared the University of Kansas Cancer Center’s approach to collaborative oncology practice, which involves detailed assessments and gap analyses. This structured approach helps identify current and future states, ensuring that partnerships are mutually beneficial and sustainable.
Warren highlighted the need for detailed contract language and collaborative governance. “The devil is in the details,” Adria explained, emphasizing the importance of clear agreements and ongoing collaboration.
Monique J. Marino is senior director of Editorial Content and Strategy at the Association of Cancer Care Centers (ACCC) in Rockville, Maryland.
References











")

: Not Traditional Telehealth Services")



















