Author(s):
BREAST CANCER IS THE MOST common cancer diagnosed among women aged 15 to 39 years in Nigeria, constituting about 50% of all cancers in that age group. Still, literature is limited on breast cancer misconceptions and knowledge gaps among undergraduate women in nonmedical fields of study in southwestern Nigeria. This study aims to address this dearth of knowledge.
Using a cross-sectional survey design, 325 nonmedical undergraduate women were selected with a stratified sampling technique. Data were analyzed employing descriptive and inferential statistical procedures. The overall knowledge of breast cancer score (total score of 48) was grouped into 3 categories: ≤16=poor, 17-32=moderate, and ≥33=good. Misconception (total score of 7) was grouped into 2:≤3=low, and ≥4=high.
The majority of the respondents were aged 16 to 25 years. The mean overall knowledge score was 34.4 ±5.46 standard deviations (SD), with 61.4% of the respondents having good overall knowledge score. The mean score for misconception was 3.2 (SD ± 1.54), with about one-third (34.6%) having a high level of misconceptions about breast cancer. Students’ ethnicity and level of study were significant predictors of breast cancer knowledge, while religion predicted breast cancer misconceptions.
Study authors concluded that there is a need for youth-friendly breast cancer awareness education within and beyond the academic community to help bridge knowledge gaps and misconceptions.
Over the years, breast cancer has received widespread attention, leading to global awareness with varying degrees of information diffusion. Early detection and advances in treatment have led to a clearer statistical picture of the disease. Nonetheless, more than a million women are diagnosed with breast cancer yearly, while thousands still die from the disease worldwide.1-5 In Africa, breast cancer mortality-to-incidence ratios are quite high. Sub-Saharan Africa has also been reported to have the worst mortality-to-incidence ratios globally.6 Estimates of age-standardized rates of breast cancer across northern Africa to western Africa ranged from 20 to 27 deaths per 100,000 women in 2020.7,8 In Nigeria, 50% of breast cancer cases result in death compared to 20% in the United States.9 In an 8-year retrospective review of data from cancer registries in Nigeria, breast cancer was the most commonly diagnosed cancer among persons aged 15 to 39 years, constituting about 50% of all cancers in that age group.1
The cause of the abnormal changes in the breast remains unknown.17 Nonetheless, several factors have been identified to be associated with the risk of developing breast cancer.18 Personal factors include age, race/ethnicity, family history/genetic background, overweight/obesity, physical inactivity, alcohol use, and smoking.19 Biological/reproductive factors include early age at menarche, use of oral contraceptives, having no children (nulliparity), not breastfeeding, having first child at a later age, hormonal exposures, late menopause, having fewer children overall, and long-term use of hormone replacement therapy.20,21 In many developing countries, urbanization and lifestyle changes have led to a marked increase in the incidence of breast cancer.2
Breast self-examination, clinical breast examination, and mammography are the most frequently used breast cancer screening practices.23 However, the benefits of breast self-examination for early diagnosis of breast cancer have been underscored in previous literature.24 It has been suggested that starting at the age of 20 years, the examination should be done monthly and performed 7 to 10 days after the first day of the menstrual cycle, when the breasts are smallest and not tender.25 Despite its benefits, low compliance with breast self-examination has been reported among female university students, especially as regards starting age and the timing of the examination.26,27 Negligence, forgetfulness, and lack of knowledge have been cited as some of the reasons for the low uptake of screening among university students.23,28
In Africa, breast cancer is more prevalent among younger and premenopausal women.29,30 However, few studies have been conducted to address the knowledge gaps and misconceptions about this disease among nonmedical undergraduate women in southwestern Nigeria. Hence, this study seeks to assess the general knowledge of breast cancer—its symptoms, risk factors, and preventive practices—as well as to identify factors that may influence both awareness and common misconceptions about the disease within this population at a private university in the region.
Hypotheses. H(01) There is no significant association between the socio-demographic characteristics of students and their overall knowledge of breast cancer.
H(02) There is no significant association between the sociodemographic characteristics of students and their level of misconception about breast cancer.
The root cause of cancer misconceptions in many resource-limited settings is a lack of knowledge.11 Common misconceptions about breast cancer have been identified, and these include that breast cancer only develops in women, is transmissible, and that it is a death sentence.5,12 Other beliefs, like cell phones and sweeteners cause cancer, have been reported among undergraduates.13 Many misconceptions about breast cancer in Nigeria are connected to ethno-religious beliefs and lower socio-economic status.14 One such misconception is the evil arrow myth, a mistaken belief that people get breast cancer from mystical sources.9,15 Knowledge of the presentations of breast cancer could increase vigilance and timely detection, which might aid the likelihood of survival. Warning signs of breast cancer include pulling in the breast, a lump in the breast or armpit, pucker/dimple/redness on breast skin, bleeding or discharge from the nipple, rash/pain in the nipple or breast skin, and changes in breast size due to swelling.16
Methods
Study Setting
This study was conducted at Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria. Afe Babalola University is a private tertiary institution located in Ado-Ekiti, Ekiti State, Southwest Nigeria. The institution offers academic programs in 5 colleges: Engineering, Law, Medicine and Health Sciences, Sciences, and Social and Management Sciences. It also has a postgraduate school and a teaching hospital domiciled within the university grounds.
Study Design
This study utilized a cross-sectional design and was conducted among undergraduate women from the Colleges of Law and Social and Management Sciences. Sample Size Determination The required sample size was calculated using Taro Yamane’s formula.31
Sample Size Determination
The required sample size was calculated using Taro Yamane’s formula.31

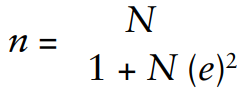
Where n is the minimum sample size required; N is the total population of students from the 2 colleges = 1627 (total population of undergraduate women in the College of Law was 856 and College of Social and Management Sciences was 771 as at the period of investigation); e is the sampling error = 0.05. Inserting these values in the above formula yielded a sample size of 321. Adjustment for a 10% rate of nonresponse yielded a final sample size of 353.
Sampling Technique
A stratified sampling technique with proportional allocation was used to recruit respondents from the Colleges of Law and Social and Management Sciences, which resulted in the selection of 186 and 167 students from the 2 colleges, respectively. Students from the 5 academic years (100 level to 500 level) were considered for the study.
Data Collection Instrument
A semi-structured questionnaire was developed to assess breast cancer knowledge, adapted from an extensive literature search. The questionnaire contained 5 sections: Section A collected data on the socio-demographic characteristics of the participants; Sections B and C assessed general knowledge of breast cancer and its symptoms; Section D evaluated knowledge of risk factors; and Section E focused on knowledge of prevention practices for breast cancer. Statements on misconceptions were integrated with knowledge items across the different knowledge groupings. The questionnaire was administered in English.
Psychometric Property and Study Variables
This study utilized measures of face and content validity. The authors and other experts examined items in the questionnaire to confirm that the intended variables were measured correctly. Testing was performed to determine the study instrument’s reliability, and a Cronbach’s alpha value of 0.78 was obtained. The independent variables were the socio-demographic characteristics of the respondents, while the dependent variables were the misconception level and overall knowledge of breast cancer.
Data Collection and Analysis
The questionnaire was uploaded with the aid of Google Forms and a short link directed to participants’ university emails and social media platforms. Data analysis was done in Statistical Package for Social Sciences (SPSS) version 23.0 (IBM Corp, Armonk, New York, US). Every correct response on general knowledge, symptoms, risk factors, and preventive practices, either a yes or a no, was awarded 1 point to obtain the total score, and every wrong response to the misconception items was given 1 point. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were calculated for study variables as appropriate. The chi-square test and logistic regression were employed for bivariate and multivariate analyses, respectively. A P value less than 0.05 was considered statistically significant. Variables were examined for multicollinearity using the variance inflation factor (VIF) diagnostic check. Multicollinearity was not present as the VIF ranged from 1.01 to 1.38 for the independent variables. Thus, the variables met the requirements for the test of significance.
Results
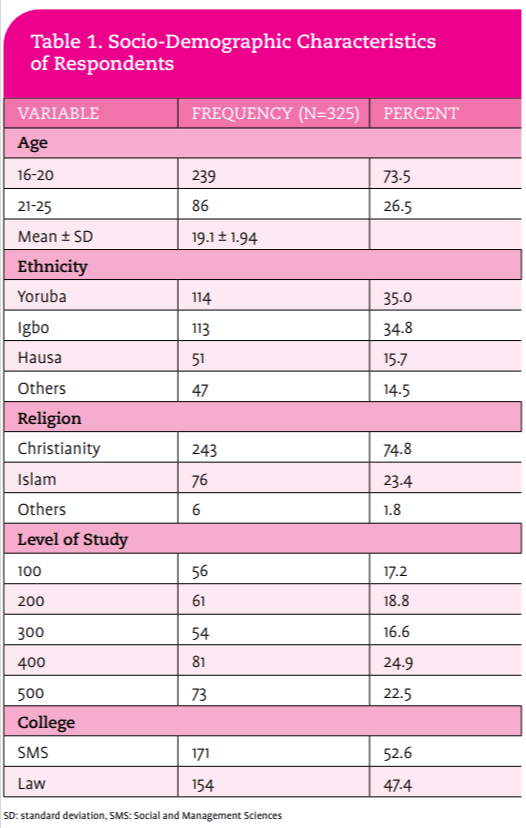
Questionnaires were filled out appropriately by 325 respondents out of a 353 calculated sample size to yield a response rate of 92.1%. Table 1, right, shows the socio-demographic characteristics of the respondents. Respondents’ ages ranged from 16 to 25 years, with a mean age of 19.1±1.94 years. Most (73.5%) respondents were within the age range of 16 to 20 years. Respondents were predominantly Christians (74.8%), while very few (1.8%) were atheists. Nearly a quarter (24.9%) of them were in their fourth year of study. Students from the College of Social and Management Sciences (52.6%) were more represented than students from the College of Law.

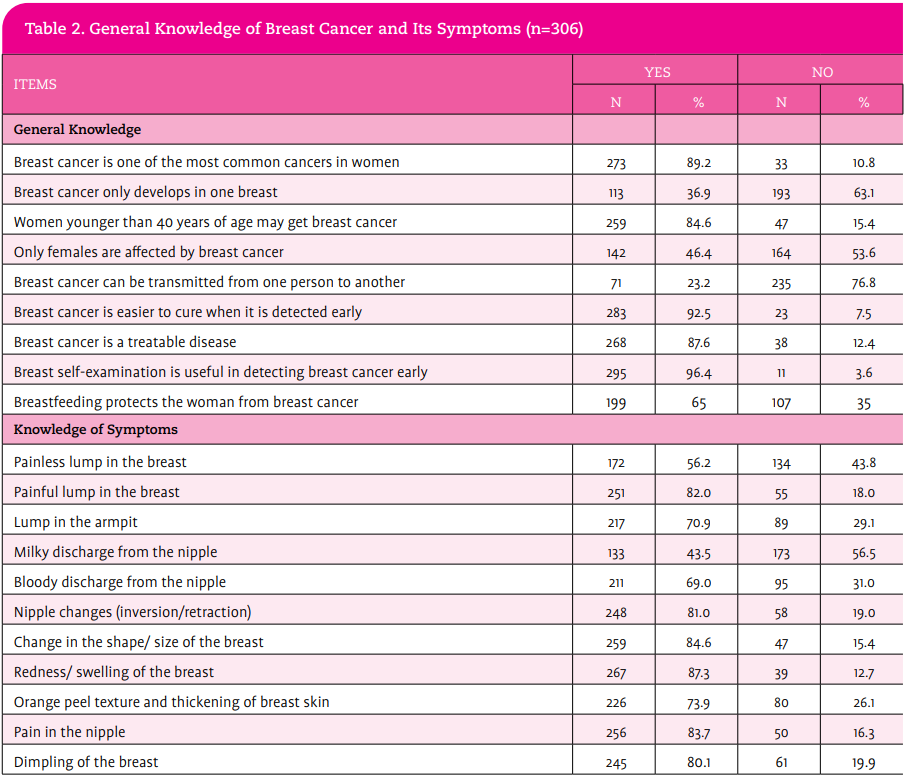
A considerable proportion (94.2%) of students were aware of breast cancer, while only 27.8% knew someone who had suffered from the disease. Most (96.4%) of those aware of the disease knew that breast self examination is useful in detecting it early. The majority of those who claimed to have knowledge of breast cancer also knew that it is easier to cure when it is detected early (92.5%) and that it is one of the most prevalent cancers in women (89.2%). About 85% were informed that women younger than 40 years of age may get breast cancer, and 86.5% knew it was a treatable disease. Over onethird (35%) of the students believed that breastfeeding does not protect a woman from breast cancer.
Table 2 shows that more than four-fifths of the students considered redness/swelling of the breast (87.3%), nipples changes (81%), changes in breast shape or size (84.6%), painful lump in breast (82%), pain in nipple (83.7%) and dimpling of breast (80.1%) as common symptoms of breast cancer. Conversely, 43.5% of students thought that milky nipple discharge was a breast cancer symptom, while 43.8% were less informed about a painless lump in the breast as a breast cancer symptom. Some common misconceptions about breast cancer were identified, including that breast cancer only affects women (46.4%), breast cancer only develops in one breast (36.9), and it is transmissible (23.2%).

The majority of students believed that health hazards such as exposing the chest region to high radiation (92.5%) was the most important risk factor for breast cancer (Table 3). Lifestyle practices such as smoking (83.7%), long-term use of hormone replacement therapy (80.1%), excessive intake of alcohol (75.2%), and frequent use of oral contraceptives (72.5%) were believed to be linked to a possible diagnosis of breast cancer among women. About half of respondents knew about important biological risk factors such as early menarche (51.3%) and late menopause (56.5%). Almost 8 out of 10 respondents opined that family history (78.4%) and personal history of breast cancer (73.2%) were also important risk factors. Common misconceptions about breast cancer risk factors included wearing underwire bras (68.6%), having large breasts (50.3%), and breastfeeding for a long time (46.4%). The majority (90.5%) of students upheld that limited oral contraceptive use and exposure of the chest region to radiation were preventive practices for breast cancer.

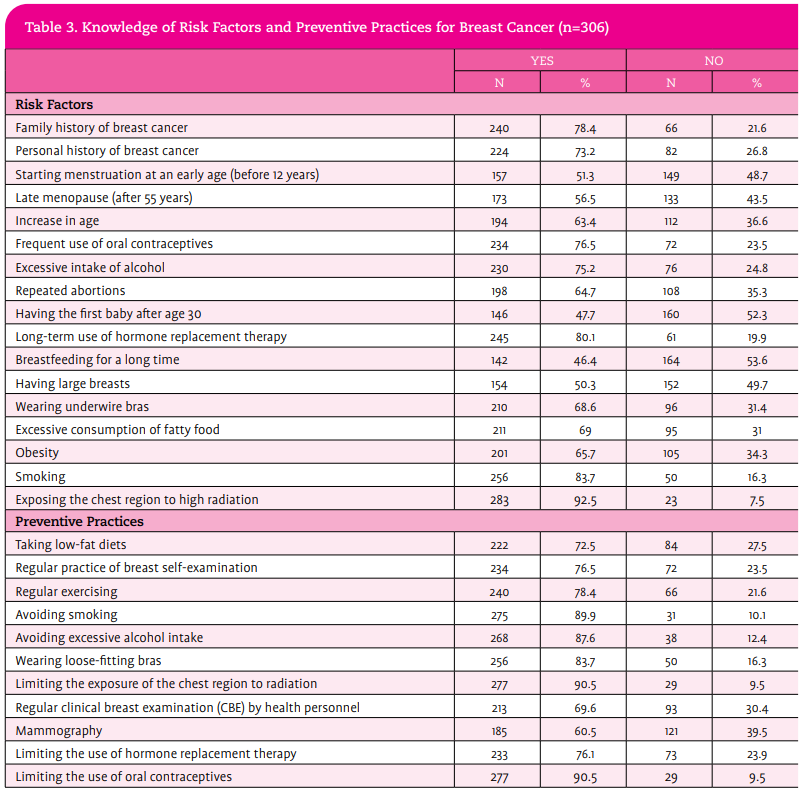
Healthy lifestyle practices such as avoiding smoking (89.9%), avoiding excessive alcohol intake (87.6%), wearing loose-fitting bras (83.7%), regular exercise (78.4%), regular practice of BSE (76.5%) alongside the limited use of hormone replacement therapy (76.1%) were believed to also prevent the development of breast cancer. Interestingly, only 3 out of 5 respondents believed that mammography (60.5%) should be employed as a preventive measure for breast cancer.
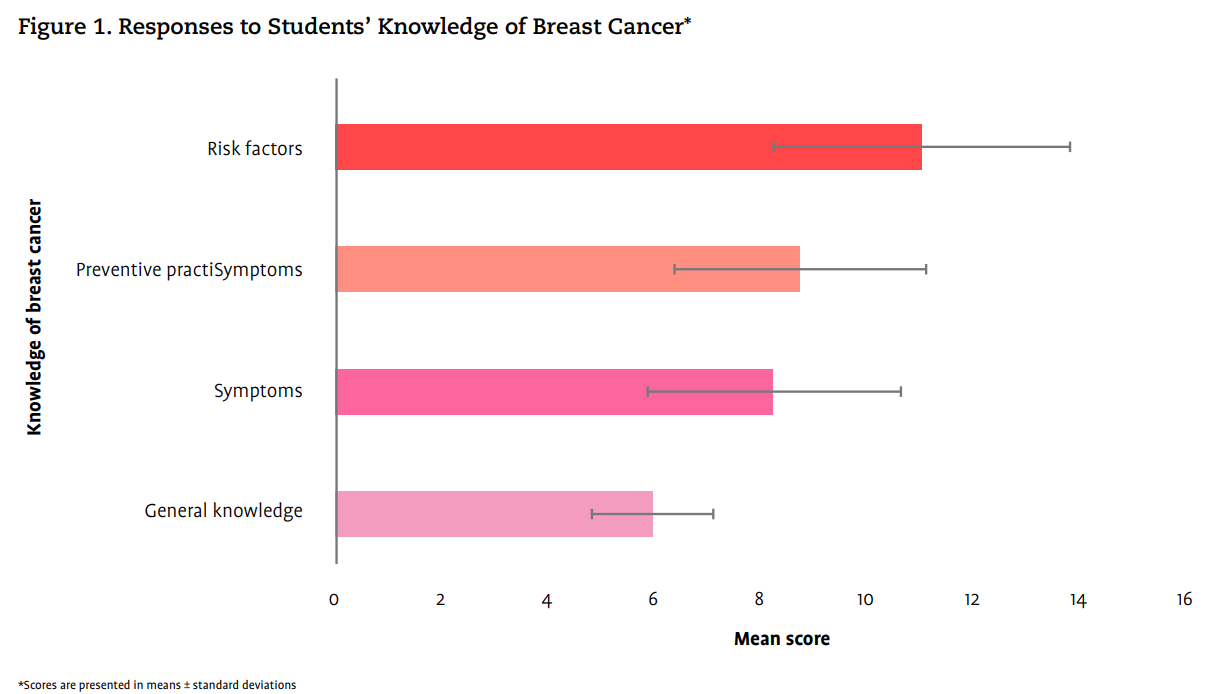
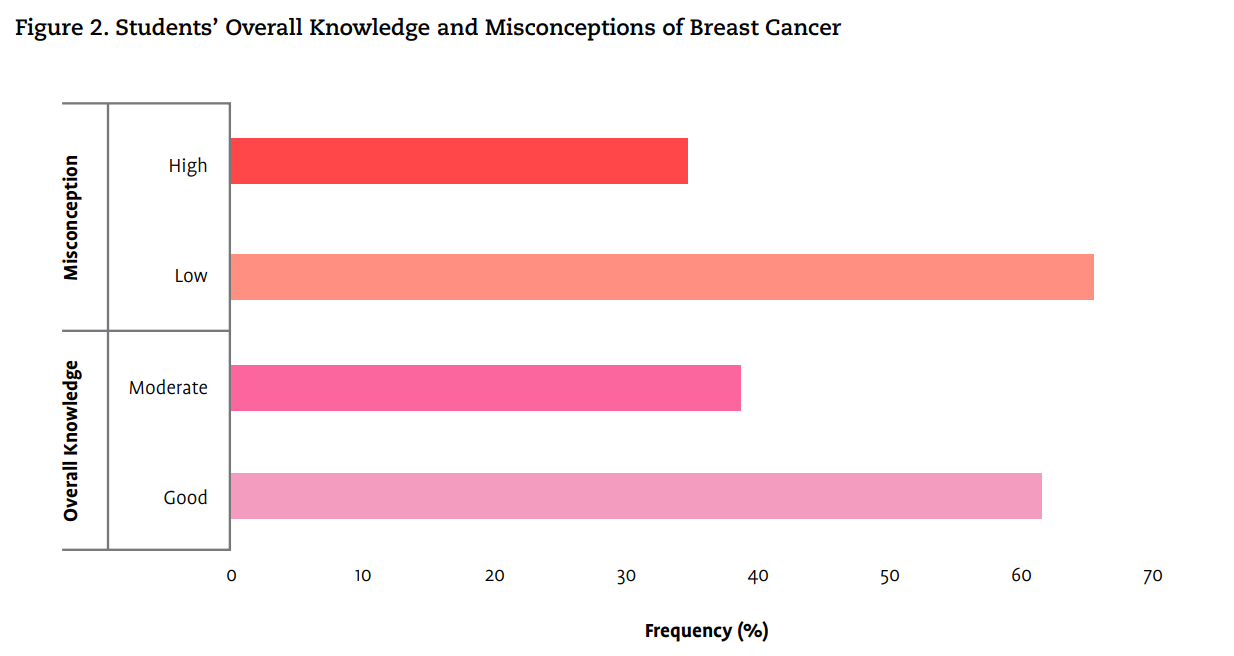
Figure 1 shows the mean scores across the different knowledge categories. The overall general knowledge mean score was 6.0 (SD ± 1.15) out of a total score of 9. None of the respondents answered all general knowledge questions about breast cancer correctly. The mean score on the knowledge of breast cancer symptoms was 8.3 (SD ± 2.4) out of a total score of 11. About 8.2% (25) of respondents obtained 100% correct responses for breast cancer symptoms. A mean score of 11.1 (SD ± 2.82) was obtained for knowledge of risk factors (total obtainable score was 17). The knowledge of preventive practices for breast cancer had a mean score of 8.8. (SD ± 2.38), the total obtainable score was 11. Students were mostly abreast of the risk factors, followed by preventive practices, symptoms, and general knowledge of breast cancer. Overall breast cancer knowledge (total score of 48) was scored into 3 groups ≤ 16=poor; 17 to 32=moderate; ≥ 33=good (Figure 2). The mean overall knowledge score was 34.2 (SD ± 6.0). A total of 188 (61.4%) respondents had good knowledge, while 118 (38.6%) had moderate knowledge. The total obtainable misconception score was 7. This was divided into 2 groups ≤3=low, and ≥ 4=high. The mean score for misconception was 3.2 (SD ± 1.54). A total of 200 (65.4%) respondents had low misconceptions, while 106 respondents (34.6%) had a high level of misconceptions about breast cancer (Figure 2).


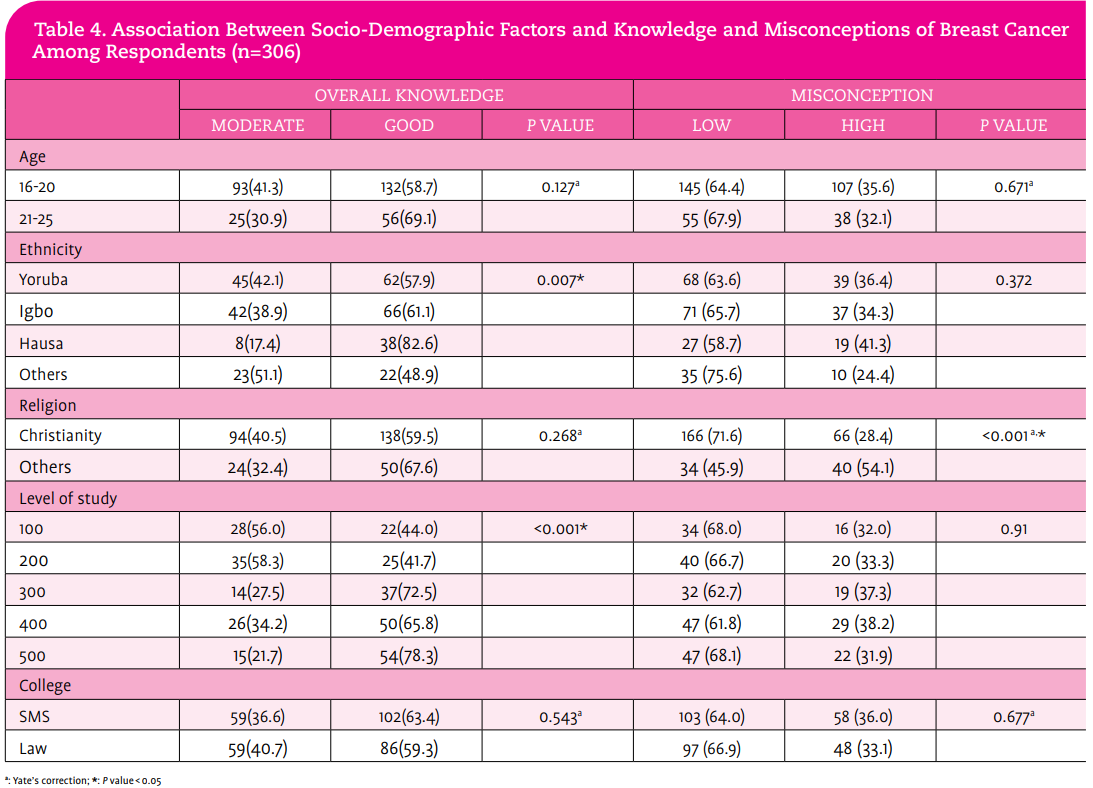
Hypotheses 1 and 2 were tested using the Pearson chi-square technique. Results revealed that ethnicity (P = .007) and level of study (P < .001) showed significant associations with students’ knowledge of breast cancer. Table 4 shows that the majority of students within each ethnic group had good knowledge of breast cancer. Similar results were obtained for students in their third to fifth year of study. However, misconceptions about the disease were only associated with religion (P < .001).

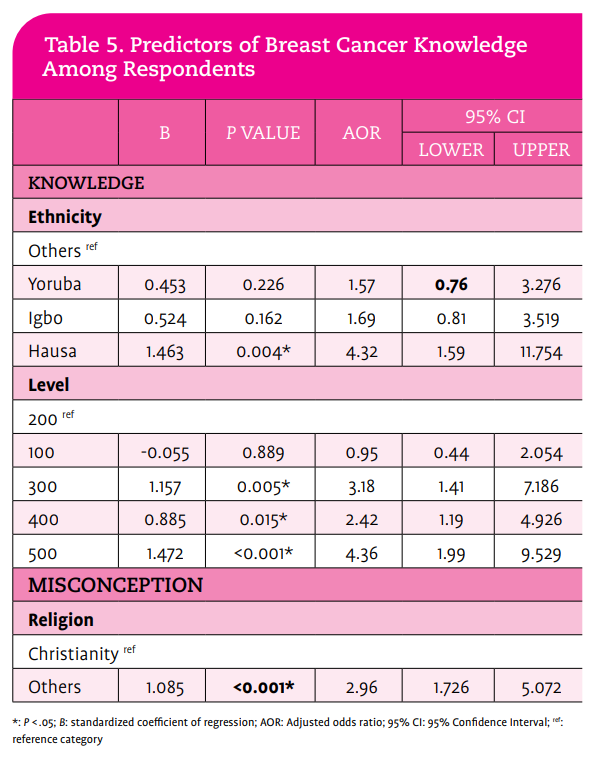
The impact of socio-demographic factors on students’ overall breast cancer knowledge and misconceptions was assessed using a logistic regression model (Table 5). While students’ ethnicity and level of study became significant predictors of knowledge of breast cancer, misconception was influenced by students’ religion. Hausa students were more likely to be knowledgeable about breast cancer than students from other tribes (AOR, 4.32; CI, 1.59-11.75). Students in higher classes—300 level (AOR, 3.18; CI, 1.41-7.19); 400 level (AOR,2.42; CI, 1.19-4.93) and 500 level (AOR, 4.36; CI, 1.99-9.53)—had better knowledge levels than those in their second year of study. Students from other religious backgrounds were more likely to have misconceptions than Christians (AOR, 2.96; 95% CI, 1.73-5.07).

Discussion
Regardless of being nonmedical undergraduate students, a considerable proportion of participants in this study were aware of breast cancer. This finding compares favorably with studies conducted among undergraduate students in Ghana and northern Nigeria, where the majority of study participants were aware of breast cancer.23,32 Moreover, good knowledge of the disease was prevalent in 61.4% of this study population. This result is in congruence with a related study carried out among undergraduate women in Osun State, Nigeria.33 Being a woman is the strongest breast cancer risk factor.5 However, approximately one half to 1% of breast cancers occur in men.12 Nearly half of the study population was unaware that breast cancer could affect men. Relatedly, this misconception had a prevalence of 41% and 52.1% in studies conducted among Ethiopian undergraduates and Iranian women, respectively.34,35
In contrast to other cancers, such as cervical cancer and human papillomavirus infection (that have infection-associated causes), the development of breast cancer has not been linked to any known microbial infection. Thus, breast cancer is not regarded as a communicable disease.5 This study’s findings revealed that nearly one quarter of students sampled felt that breast cancer is transmissible. Lower and higher misconceptions (13% versus 81%) about breast cancer transmission have been documented in research conducted outside and within a school-based population.34-36 More than fourfifths of study participants considered redness/swelling of the breast, nipple changes, change in breast shape or size, painful lump in the breast, pain in the nipple, and dimpling of the breast as common symptoms of breast cancer. However, more than two-fifths of them were unaware that a painless lump in the breast may be a presentation of the disease. These results agree with reports among university students from south Nigeria, where 31% were unaware.37
Surprisingly, the majority of the study population believed that exposing the chest region to radiation and smoking were the most vital risk factors for breast cancer. Disruption in the biological clock, such as early menarche, late menopause, and hormonal therapy, are important factors responsible for an increased risk of breast cancer in women.38,39 Yet, nearly half of students interviewed were inadequately informed about early menarche and late menopause as risk factors. A similar result was observed among university students in Togo and Sylhet, Bangladesh.16,40 Being knowledgeable about breast cancer preventive practices may assist young women in taking appropriate measures early. This study found that a large proportion of students upheld that the limited use of oral contraceptives and exposure of the chest region to radiation were major preventive practices. Interestingly, only 3 out of 5 respondents were aware of mammograms as a modality for breast cancer screening. A better knowledge level was identified among Saudi Arabian women, where 71% were informed of mammography as a preventive measure for breast cancer.18
The knowledge gap observed across the different knowledge aspects in this study suggests the need to improve awareness regarding breast cancer symptoms and general knowledge among students. The level of knowledge was higher for risk factors than for preventive practices and symptoms of breast cancer. Consistent with this study is a report from undergraduate women in Bangladesh, where knowledge of symptoms was less than that of risk factors.41 Nonetheless, the current study’s findings are unlike a report among young women in Iran, where the level of knowledge of symptoms was higher than risk factors.35,42 A possible reason for the variance in knowledge gaps could be attributed to the fact that the Iranian studies captured a general population of women, with older women who might have had some degree of exposure and education as regards the symptoms of breast cancer.
Understanding the factors influencing the knowledge and misconceptions about a disease is invaluable for informing sustainable and effective interventions in the community. In the present study, the level of education and ethnicity determined students’ knowledge of breast cancer. This outcome could be a result of increased exposure and acquaintance with breast cancer and other related health issues as the students advance academically. The impact of students’ level of study on breast cancer knowledge has been upheld in similar studies conducted within and outside Africa.34,41 Religion was the single determinant of participants’ misconceptions of breast cancer in this study. This finding is not unanticipated, considering the ethnoreligious diversity of the study setting. Nonetheless, these barriers should be a consideration for health care professionals to play a more prominent role in enlightening young women about breast cancer and also encouraging them to participate in precautionary and screening programs.
As with any study, this study is not exempt from limitations. First, this study employed a cross-sectional design. Thus, the breast cancer knowledge levels and gaps among respondents might not truly reflect the actual situation over a period of time. Secondly, this study included students from a single private university. Therefore, the results should be interpreted carefully, as they may not reflect the knowledge and misconceptions of the women’s student population in southwestern Nigeria. Nevertheless, these study findings add additional knowledge to the growing body of research in this field.
Conclusion
This study concluded that well over three-fifths of undergraduate women had an overall good knowledge of breast cancer, while a high misconception level was prevalent in more than one-third. Also, knowledge gaps were observed, particularly in the general knowledge of the disease, including its symptoms, preventive practices, and risk factors. Whereas ethnicity and level of study became significant predictors of knowledge of breast cancer, misconception was influenced by students’ religion. Interestingly, this study population consists of women currently enrolled at a university, and one would assume that they have access to the most recent health information. The knowledge gaps and misconceptions about breast cancer observed in this group suggest the likelihood that such issues may be even more pronounced among women without a university or tertiary education. This study highlights the need for appropriate and adequate youth-friendly services to support breast cancer awareness and screening programs both within and beyond the university community.
Acknowledgment: The authors wish to thank all students who took part in this study.
Authors’ Contributions: RIF and GMO designed and implemented the study. All authors were involved in the literature search. OEA analyzed the data and wrote the first draft of the manuscript. OEA and AF interpreted the results. RIF, OEA, and AF revised the manuscript. All authors read and approved the final version of the manuscript.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement: The datasets produced and analyzed during this study are available from the corresponding author on reasonable request.
Conflicts of Interest: The authors declare no conflicts of interest.
Ethical Approval: Ethical approval (AB/EC/21/02/169) was obtained from the Research and Ethics Committee of Afe Babalola University. Participants were fully informed about the nature of the study and what findings needed to be obtained. Informed consent was obtained as participants were informed of their right to voluntary participation or withdraw from the study at any point. Confidentiality, anonymity, and privacy were also ensured.
Risikat Idowu Fadare, is a registered midwife educator and lecturer in the Department of Nursing Science, College of Medicine and Health Sciences at Afe Babalola University in Ado-Ekiti, Nigeria. Oluwaseun Eniola Adegbilero-Iwari is a bio-statistician in the Department of Community Medicine, College of Medicine and Health Sciences at Afe Babalola University in Ado-Ekiti, Nigeria. Goodness Mary Odu is with the Department of Nursing Science, College of Medicine and Health Sciences at Afe Babalola University in Ado-Ekiti, Nigeria. Ayodeji Fasoro is a research fellow in the Department of Public Health at the University of Otago in Wellington, New Zealand.
References
1. Houshian R. Level of knowledge about breast cancer risk factors and early detection among baccalaureate nursing students. Master’s thesis. California State University; 2017. Accessed June 22, 2025. https://scholarworks.calstate. edu/downloads/9k41zf14w
2. Osei E, Osei Afriyie S, Oppong S, Ampofo E, Amu H. Perceived breast cancer risk among female undergraduate students in Ghana: a cross-sectional study. J Oncol. 2021;2021(1):8811353. https://doi. org/10.1155/2021/8811353
3. Lei S, Zheng R, Zhang S, et al. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020. Cancer Commun. 2021;41(11):1183-1194. https://doi.org/10.1002/ cac2.12207
4. Soerjomataram I, Bray F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nat Rev Clin Oncol. 2021;18(10):663-672. doi:10.1038/s41571-021-00514-z
5. World Health Organization. Breast Cancer. March 13, 2024. Accessed April 17, 2025. https://www.who.int/news-room/fact-sheets/detail/ breast-cancer
6. Martei YM, Dauda B, Vanderpuye V. Breast cancer screening in sub-Saharan Africa: a systematic review and ethical appraisal. BMC Cancer. 2022;22(1):203. doi:10.1186/s12885-022-09299-5
7. Hercules SM, Alnajar M, Chen C, et al. Triple-negative breast cancer prevalence in Africa: a systematic review and meta-analysis. BMJ Open. 2022;12(5):e055735. doi:10.1136/bmjopen-2021-055735
8. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
9. Sarki AM, Roni BL. This disease is “not for hospital”: myths and misconceptions about cancers in Northern Nigeria. J Glob Health Rep. 2019;3:e2019070. doi:10.29392/joghr.3.e2019070
10. Ntekim A, Oluwasanu M, Odukoya O. Breast cancer in adolescents and young adults less than 40 years of age in Nigeria: a retrospective analysis. Int J Breast Cancer. 2022(1):9943247. doi:10.1155/2022/9943247
11. Biswas J. Debunk the myths: oncologic misconceptions. Indian J Med Res. 2014;139(2):185-187. https://pmc.ncbi.nlm.nih.gov/articles/ PMC4001327/
12. Cancer Research UK. Breast cancer in men. Accessed April 17, 2025. https://www.cancerresearchuk.org/about-cancer/breast-cancer/types/ male-breast-cancer
13. Domínguez M, Sapiña L. From sweeteners to cell phones-cancer myths and beliefs among journalism undergraduates. Eur J Cancer Care (Engl). 2020;29(1):e13180. doi:10.1111/ecc.13180
14. Anugwom K. Social and institutional support in breast cancer management among elderly women in Nigeria. In: Anugwom EE, Awofeso N, eds. Public Health in Developing Countries - Challenges and Opportunities. IntechOpen; 2019.
15. Ololade KO, Alabi A, Fadipe B, Adegboyega B. The ‘evil arrow’ myths and misconceptions of cancer at Lagos University Teaching Hospital, Nigeria. S Afr J Onco. 2019;3(0):a49. doi:10.4102/sajo.v3i0.49
16. Akter MF, Ullah MO. Awareness levels of breast cancer among female university and medical college students in Sylhet city of Bangladesh. Cancer Rep. 2022;5(11):e1608. doi:10.1002/cnr2.1608
17. National Breast Cancer Foundation. Breast cancer risk factors. Accessed April 17, 2025. https://www.nationalbreastcancer.org/ breast-cancer-risk-factors/
18. Gari A, Khayyat S, Khushaim L. Awareness of breast cancer screening and risk factors among the general female population in the Western Province of Saudi Arabia: a cross-sectional study. J Med Res Surg. 2022;3(2):19-30. doi:10.52916/jmrs224071
19. Smith RA, Manassaram-Baptiste D, Brooks D, et al. Cancer screening in the United States, 2015: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2015;65(1):30-54. doi:10.3322/caac.21261
20. Younis M, Al-Rubaye D, Haddad H, Hammad A, Hijazi M. Knowledge and awareness of breast cancer among young women in the United Arab Emirates. ABCR. 2016;5(4):163-176. doi: 10.4236/abcr.2016.54019
21. Akoko LO, Rutashobya AK, Lutainulwa EW, Mwanga AH, Kivuyo SL. The effect of reproductive, hormonal, nutritional and lifestyle on breast cancer risk among black Tanzanian women: A case control study. PLoS One. 2022;17(2):e0263374. doi:10.1371/journal.pone.0263374
22. Antony MP, Surakutty B, Vasu T, Chisthi M. Risk factors for breast cancer among Indian women: A case–control study. Niger J Clin Pract. 2018;21(4):436-442. doi:10.4103/njcp.njcp_102_17
23. Ossai EN, Azuogu BN, Ogaranya IO, Ogenyi AI, Enemor DO, Nwafor MA. Predictors of practice of breast self-examination: a study among female undergraduates of Ebonyi State University, Abakaliki, Nigeria. Niger J Clin Pract. 2019;22(3):361-369. doi:10.4103/njcp.njcp_482_18
24. Hamed E, Alemrayat B, Syed MA, Daher-Nashif S, Rasheed HMA, Kane T. Breast cancer knowledge, attitudes and practices amongst women in Qatar. Int J Environ Res Public Health. 2022;19(7):3995. doi:10.3390/ ijerph19073995
25. Muchirevesi SS. Knowledge and practices of breast self-examination among women admitted at a private clinic, Zimbabwe. Master’s thesis. University of South Africa; 2016. Accessed April 17, 2025. http://hdl.handle. net/10500/22589
26. Salawu MM, Akindiya OE. Practice of breast self-examination among female undergraduate students of Adeleke University, Ede, Osun State. Res J Health Sci. 2018;6(4):157-163. doi:10.4314/rejhs.v6i4.1
27. Ahmed MS, Sayeed A, Mallick T, Syfuddin HM. Knowledge and practices on breast cancer among Bangladeshi female university students: a cross-sectional study. Asian Pac J Cancer Care. 2020;5(1):19-25. doi:10.31557/apjcc.2020.5.1.19-25
28. Tewabe T, Mekuria Z. Knowledge and practice of breast self-examination among undergraduate student in Bahir Dar University, North-West Ethiopia, 2016: A cross-sectional study. J Public Health Afr. 2019;10(1):805. doi:10.4081/jphia.2019.805
29. Azubuike SO, Muirhead C, Hayes L, McNally R. Rising global burden of breast cancer: the case of sub-Saharan Africa (with emphasis on Nigeria) and implications for regional development: a review. World J Surg Oncol. 2018;16(1):63. doi:10.1186/s12957-018-1345-2
30. Getu MA, Abebe M, Tlaye KG, Goshu AT. Breast Self-Examination Knowledge and its Determinants among Female Students at Addis Ababa University, Ethiopia: An Institution-Based Cross-Sectional Study. BioMed Research International. 2022;2022(1):2870419. doi:10.1155/2022/2870419
31. Yamane T. Statistics: An Introductory Analysis. Harper & Row; 1967.
32. Saulawa HT, Auwal FI, Danjuma NM. Knowledge and awareness of breast cancer risk factors and screening methods amongst undergraduate pharmacy students of Ahmadu Bello University Zaria, Nigeria. Nig J Pharm Res. 2022;18(1):55-62. doi:10.4314/njpr.v18i1.6
33. Olufemi OO, Omowumni SR, Ajoke OA, Olufemi AE. Knowledge and awareness of breast cancer and screening methods among female undergraduate students in a semi-urban college of culture and humanities, Nigeria. Int J Caring Sci. 2017;10(1):88-99.
34. Gebresillassie BM, Gebreyohannes EA, Belachew SA, Emiru YK. Evaluation of knowledge, perception, and risk awareness about breast cancer and its treatment outcome among University of Gondar students, Northwest Ethiopia. Original Research. Front Oncol. 2018;8:501. doi:10.3389/ fonc.2018.00501
35. Moridi A, Mahmoodi S, Rahmati N, Fathi M, Naeiji Z. Comparison of awareness level about breast cancer risk factors, presentations, and screening rules and tools: a cross-sectional study on general female population. J Obstet Gynecol Cancer Res. 2021;6(4):188-194. doi:10.30699/jogcr.6.4.188
36. Esan DT, Ogar IM, Fasoro A, Esan TO, Oluwafemi F, Odesanya OE. Knowledge and practice of breast cancer screening among healthcare professionals in a tertiary health institution in Nigeria. IOSR JNHS. 2016;5(3):132-138. doi:10.9790/1959-050303132138
37. Onwusah DO, Eboigbe MU, Arute JE, Mgbahurike AA. Knowledge and awareness of breast cancer among university students in South-South Nigeria. Sch Acad J Pharm. 2017;6(1):4-15.
38. McPherson K, Steel CM, Dixon JM. ABC of breast diseaes. Breast cancer–epidemiology, risk factors, and genetics. BMJ. 2000;321(7261):624- 628. doi:10.1136/bmj.321.7261.624
39. Akram M, Iqbal M, Daniyal M, Khan AU. Awareness and current knowledge of breast cancer. Biol Res. 2017;50(1):33. doi:10.1186/ s40659-017-0140-9
40. Heena H, Durrani S, Riaz M, et al. Knowledge, attitudes, and practices related to breast cancer screening among female health care professionals: a cross sectional study. BMC Womens Health. 2019;19(1):122. doi:10.1186/ s12905-019-0819-x
41. Sarker R, Islam MS, Moonajilin MS, Rahman M, Gesesew HA, Ward PR. Knowledge of breast cancer and breast self-examination practices and its barriers among university female students in Bangladesh: findings from a cross-sectional study. PLoS One. 2022;17(6):e0270417. doi:10.1371/journal. pone.0270417
42. Tilaki KH, Auladi S. Awareness, attitude, and practice of breast cancer screening women, and the associated socio-demographic characteristics, in northern Iran. Iran J Cancer Prev. 2015;8(4):e3429. doi:10.17795/ijcp.3429