Author(s):
FROM 2010 TO 2019, the Association of Cancer Care Centers (ACCC) fielded an annual Trending Now in Cancer Care Delivery survey to its membership to gain insights into challenges faced and—most importantly—solutions to address those challenges. When its busy provider members shared the challenges involved in taking this time- and resource-intensive survey, ACCC identified alternate ways to collect these data, including at the ACCC 51st Annual Meeting & Cancer Center Business Summit (AMCCBS). Beginning in 2023, ACCC hosted a series of interactive sessions on hot topic areas impacting oncology providers and cancer care delivery. Insights and solutions from discussions at AMCCBS 2025 were used to develop this report; prior reports are available on the ACCC website.


Facilitators
Lessons From Implementing the Living Well Program
At AMCCBS 2025, Dr. Mariusz Wirga challenged the status quo of cancer care. His message was clear: “Mental health is a cancer survival issue.” Dr. Wirga’s journey began in the 1980s. He was inspired by the groundbreaking work of Dr. Carl Simonton, who demonstrated that psychological support could improve both the quality of life and survival rates for patients with cancer. “I started running support groups while still in my pathology residency,” Dr. Wirga recalled. “I saw the distress in patients and knew I had to do more.” This early experience led him to psychiatry, and he embraced cognitive behavioral therapy as a cornerstone of his approach. Over the years, he developed the Beat the Odds program, a structured, skills-based intervention that has helped thousands of patients cope with the emotional toll of cancer.
Dr. Wirga painted a sobering picture of the current state of psycho-oncology. While only 10% to 13% of the general population experience depression or anxiety, over 55% of patients with cancer suffer from these conditions—yet fewer than 5% receive appropriate care. “This is not just a gap,” he emphasized. “It’s a chasm.”
The consequences are severe. Patients with untreated mental health issues are more likely to experience longer hospital stays, higher emergency department (ED) visits, and increased readmission rates. “It costs over $120,000 more to treat a cancer patient with unaddressed mental health concerns,” Dr. Wirga explained. “And that’s not just dollars—it’s lives.”
The failure, according to Dr. Wirga, is both systemic and cultural. On the provider side, there is a lack of awareness and education about the importance of mental health in oncology. “Mental health is not part of the protocol,” he said. “And it should be.”
Patients, too, face barriers. Many believe they are coping as best they can, and they are unaware that coping skills can be taught and improved. Families and even health care providers often normalize distress, saying, “Of course they’re depressed—they have cancer.” This mindset, Dr. Wirga argued, reinforces stigma and prevents patients from seeking help.
Access is another major hurdle. There are not enough trained mental health professionals, and services are often not reimbursed. “It’s treated as a pure cost,” he argued. “As if the mind were separate from the body.”
A Digital Solution: The Living Well Program
To address these challenges, Dr. Wirga and his collaborators developed the Living Well program—a digital, tiered model of care that delivers cognitive behavioral therapy through a mobile app. “We needed something scalable, accessible, and evidence-based,” he said. “And we found it.”
The Living Well app is more than a wellness tracker—it’s a clinically grounded therapeutic tool. It offers 24/7 access to structured cognitive behavioral therapy modules that help patients reframe negative thoughts, manage stress, and build emotional resilience. “It’s not just mindfulness or breathing exercises,” Dr. Wirga noted. “It’s real therapy—targeted, structured, and effective.”
The app includes built-in distress monitoring, which tracks emotional states and alerts users when intervention may be needed. It features a tiered support system: all patients receive universal access to the app, moderate-risk users can connect with trained coaches, and high-risk individuals are referred to licensed therapists or psychiatrists, often via telehealth.
One of the app’s most powerful features is its ability to act as a gateway to therapy. “We found that patients who started with the app were more likely to seek professional support,” Dr. Wirga said. “[The technology] lowers the barrier to entry.”
“Those who were most anxious and depressed at the start saw the greatest improvements,” Dr. Wirga said. “That’s the power of early, targeted intervention.”
The financial implications are equally compelling. By reducing ED visits and improving treatment adherence, the program can save over $6.4 million per 1000 patients annually. “It’s not just good medicine,” Dr. Wirga concluded. “It’s smart economics.”
Multiple studies across the US, Poland, and Germany have validated the program’s effectiveness.
A Game-Changer for Patients and Providers
The impact on patients has been profound. Patients using the Living Well app showed significant reductions in anxiety, depression, and distress. In a randomized controlled trial at the MemorialCare Todd Cancer Institute, patients who used the app maintained stable emotional health, while those in the control group experienced worsening symptoms. Patients also reported feeling more empowered and in control of their treatment journey. “It gave me tools I didn’t know I needed,” a patient told Dr. Wirga in a testimonial. “I could finally sleep through the night without waking up in panic.” Use of the app also improved treatment adherence, with more patients following through with their prescribed treatment plans, potentially improving survival outcomes.
For health care providers, the app offers a scalable solution to a long-standing problem. It reduces the burden on overextended mental health professionals by triaging patients based on need. “It optimizes our resources,” Dr. Wirga explained. “Psychologists can focus on the patients who need them most.” The app also integrates with electronic health records (EHRs), allowing for seamless referrals and real-time monitoring. Providers receive alerts when a patient’s distress levels spike, enabling timely intervention. “It’s like having a digital assistant that never sleeps,” an oncologist in the audience remarked. The Living Well app also supports value-based care models by improving outcomes and reducing costs. “This is where digital psycho-oncology can thrive,” Dr. Wirga said. “It’s where we can finally bridge the gap between mind and body.”
Key Takeaways for Cancer Programs
For cancer programs looking to replicate the success of the Living Well program, Dr. Wirga offered several actionable insights:
Dr. Wirga ended his presentation with a powerful call to action for those in the room, stating, “Let’s make digitally enabled psycho- oncology the new standard. Let’s stop treating mental health as an afterthought and start treating it as essential to survival.”
A Value-Based Model for Early Palliative Care in Advanced Cancer
As a caregiver, seasoned health economist, and 2-time cancer survivor, Torrie Fields brought a unique blend of data-driven insight and personal experience to the conversation—the urgent need to integrate early palliative and supportive care into cancer treatment. Fields began by clarifying a common misconception. Palliative care is not synonymous with end-of-life care. “Palliative care is a preventive service,” she explained, “focused on improving quality of life by anticipating, preventing, and treating suffering—physical, emotional, social, and spiritual.” Supportive care, she added, is the broader umbrella that includes services like psychosocial support, financial counseling, and care coordination throughout the cancer journey. This distinction is critical. While supportive care can be delivered by a range of professionals, palliative care is a recognized medical sub-specialty. Despite overwhelming evidence of its benefits to patients, however—including improved quality of life, reduced symptom burden, better treatment adherence, and even longer survival—access to these services remains limited.

The Evidence Is Clear—But Action Lags
Fields highlighted a troubling paradox as she noted, “We know palliative care works. We know it saves money. And yet, most patients never receive this care.” She pointed to a fragmented system in which reimbursement models, workflow barriers, and lack of awareness prevent timely referrals. For example, while advance care planning and palliative consultations are reimbursed under Medicare, inter-disciplinary palliative care services—including nursing, social work, and spiritual support—are not. “Unless you’re dying enough to qualify for hospice,” Fields explained, “you fall into a [care] gap. I know, because I did.” She recounted her own experience with stage 3B cervical cancer—despite her professional background in value-based care, she struggled to access the very services she had helped design. “My oncologist had nowhere to refer me. I wasn’t dying, but I wasn’t okay either.”
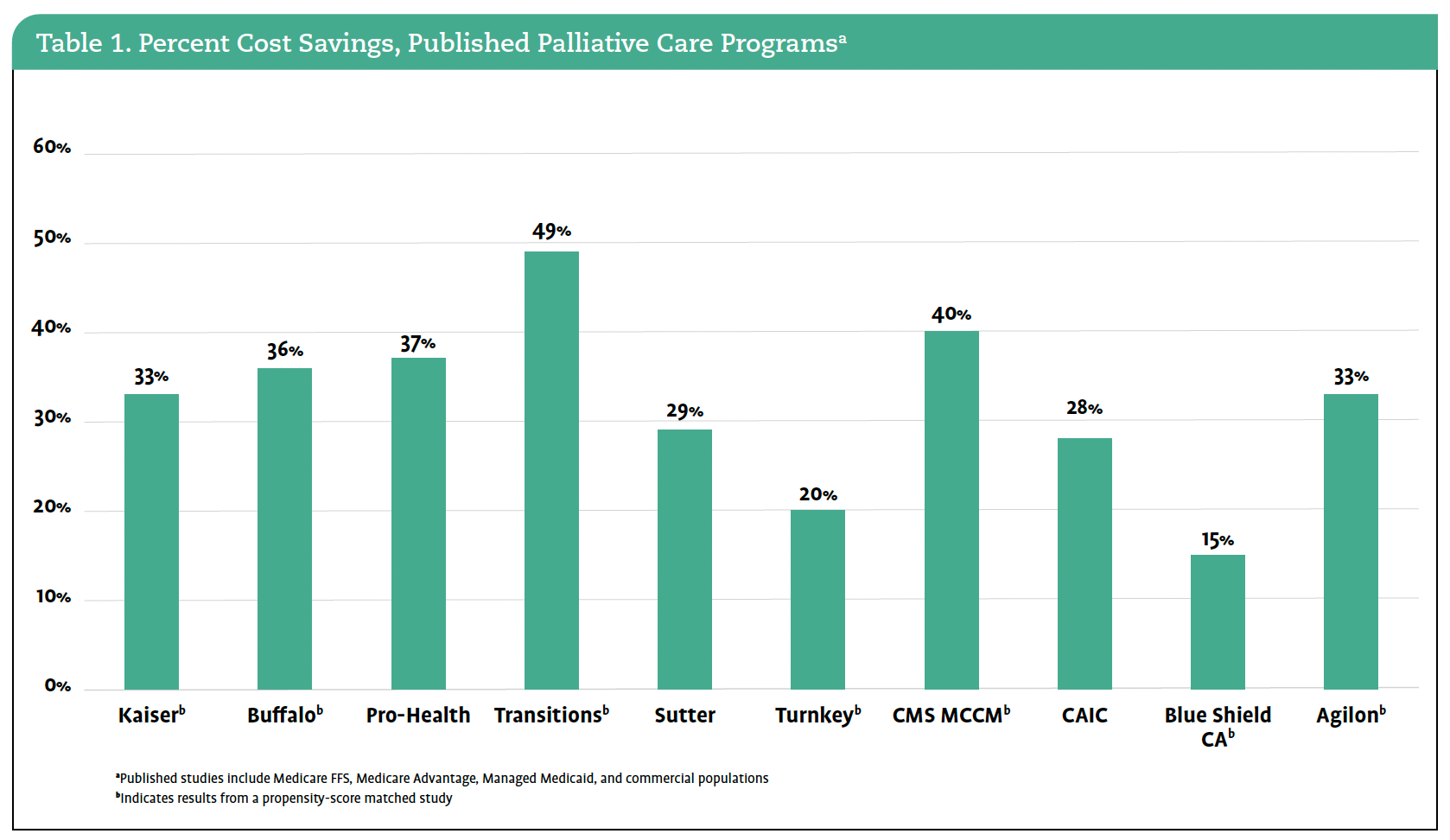
Fields reviewed decades of research, including landmark studies by Jennifer Temel2 and others,3 showing that early palliative care improves outcomes and reduces costs. She cited data from the Centers for Medicare & Medicaid Service’s (CMS) Oncology Care Model that showed 33% of cost savings attributed to embedded palliative care; private insurers have also published studies showing up to 49% reductions in total cost of care (Table 1).
Despite this evidence, adoption remains low. “Choosing Wisely guidelines have been out since 2011,” Fields noted, “but we still see chemotherapy in the last 2 weeks of life and low hospice utilization. This isn’t just a financial problem—it’s a workflow problem.”
The Workflow Problem
“Even when oncologists want to refer patients to palliative care, they often don’t know when or how to do it,” Fields explained. “There’s no standardized referral process, and the terms—supportive care, palliative care, hospice—are often misunderstood or used interchange-ably. That confusion creates hesitation.”
One of the most significant barriers is the lack of integration into EHRs. Without built-in prompts or referral pathways, palliative care becomes an extra step in an already overburdened clinical workflow. “We’re asking providers to do more without giving them the tools to do it efficiently,” Fields said.
Additionally, many clinicians are unaware of which services are reimbursable or ways to bill for these services. For example, advanced-care planning is reimbursed under Medicare, but if it is initiated by a specialist like an oncologist, it may trigger a co-pay for the patient—creating a disincentive for doing the right thing. “There’s a disconnect between what’s clinically appropriate and what’s operationally feasible,” Fields noted. “We’ve built a system that rewards volume, not value, and that makes it hard for providers to prioritize whole-person care.”
How Palliative Care Benefits Patients and Providers
Fields emphasized that palliative care is not just about comfort at the end of life—it’s about helping people live better with serious illness.
“It’s about managing pain, anxiety, depression, and caregiver burn-out,” she said. “It’s about giving people the tools to make informed decisions and access the treatments that are right for them.” Patients who receive palliative care experience:
The benefits extend beyond patients. For providers, palliative care offers:
Fields noted that many oncologists want to refer patients to palliative care but are unsure when or how to do so. “We need to make it easier,” she said. “That means building referral pathways, training staff, and embedding these services into routine care.”
The Value in Supportive Cancer Care Project
To address these challenges, Fields worked with the Together for Supportive Cancer Care Coalition to launch the Value in Supportive Cancer Care initiative—an 18-month quality improvement project designed to implement and evaluate a standardized referral pathway for supportive and palliative care. The initiative is grounded in 4 goals:
The project is being piloted in 4 states—Ohio, Utah, North Carolina, and New Jersey—with participation from both community and academic cancer centers. Health plans also are developing bundled payment models that reflect the true value of supportive care. The evaluation framework includes a balanced scorecard of outcomes:
“This isn’t a clinical trial,” Fields emphasized. “It’s real-world implementation. We’re not testing whether palliative care works—we know it does. We’re testing how to make it work in practice.” She also wants to hear from cancer programs that are not currently participating in the pilot. “If you are not in Ohio, Utah, North Carolina, or New Jersey, I’d love to hear about your experiences with supportive care and palliative care and how we can learn lessons from the initiatives you’ve already done.”
Fields closed with a moving slide showing her family—herself, her partner recently diagnosed with glioblastoma, and 3 loved ones she has cared for through cancer. “None of us were ever offered palliative care,” she said. “We thought the system would take care of us. It didn’t.” Her message was clear as she commented, “We’ve known the answer for over a decade. Now it’s time to act.”
Making the Case for Whole-Person Navigation in Oncology
Founded in 2018, the American Oncology Network (AON) has grown into a national network of over 100 locations across 20 states, operating under a single tax identification number. This structure allows for centralized innovation and respects the unique design and needs of individual practices. “We’re a supergroup with local nuance,” Anne Marie Rainey explained. “That means we can think big, but we have to implement smart.” AON has long been committed to value-based care, participating in the Oncology Care Model, the Enhancing Oncology Model (EOM), and several commercial payer programs. These experiences have shaped AON’s approach to care coordination, social determinants of health (SDOH) screening, and, now, principal illness navigation (PIN).
Why Principal Illness Navigation (PIN)?
PIN is a relatively new CMS-reimbursable service designed to address the non-medical barriers that often derail cancer treatment—transportation issues, financial stress, food insecurity, and more. “We already do this work,” Rainey said, “through nurse triage, social workers, patient and financial navigators, and dietitians. PIN just gives us a framework—and a funding stream—to do it better.” PIN services include:
PIN billing codes require documentation, time tracking, and trained personnel. “AON is using social workers, nurse navigators, and lay navigators trained through the George Washington Cancer Navigation program,” Rainey noted. To scale PIN across its network, AON partnered with Vantage Technologies to implement Social Health 360, a cloud-based platform that supports documentation, timekeeping, and integration with AON’s EHR. “We needed a low-tech, high-impact solution,” Rainey said. “And we needed it to be flexible enough to work across diverse practice settings.”
PIN rollout began with a pilot phase, prioritizing AON practices with existing navigation staff, high area deprivation index scores, and/or recent natural disasters. As of spring 2025, PIN services are active in Arkansas, Ohio, North Carolina, Hawaii, Georgia, and Indiana—with Missouri and Iowa soon to follow.
Rainey made a compelling case for why cancer programs should not only implement PIN services but also ensure they are billing for these services:
Barriers and Challenges to Implementing PIN Services
When its team set out to implement PIN services, AON knew it wouldn’t be easy. “This is hard work,” Rainey admitted during her presentation. “It’s not just about adding a billing code—it’s about transforming how we deliver care.” The challenges began with change management. Convincing clinical teams across more than 100 locations to adopt new workflows, track time, and document services in unfamiliar ways required more than just training—it required trust. Some practices embraced the change quickly, while others needed more time and support. “Every practice is different,” Rainey explained. “We had to be flexible and creative.”
Technology was another hurdle. AON’s existing EHR was not equipped to handle the documentation and timekeeping required for PIN billing. Social Health 360 helped AON bridge this gap. Even so, integration was not seamless. The team had to adjust HL7 feeds (a stream of electronic health data transmitted between different health care systems using the Health Level Seven standards), reformat PDF outputs, and rework billing processes to ensure everything flowed correctly. “Virtual training doesn’t always cut it,” Rainey admitted. “We’ve found that in-person support is key to building confidence and consistency.”
Billing itself presented a unique set of challenges. PIN services are reimbursed through a series of codes; however, as stated above, these services often require patient co-pays. Some insurance plans charged patients up to $50 for a service that reimburses providers around $78.
Staffing and workflow variation across AON’s vast network added another layer of complexity. Some practices used nurse navigators, whereas others employed lay navigators or social workers. Each practice had its own way of doing things, which made standardization difficult. “We had to analyze workflows practice by practice,” Rainey said. “It was the only way to ensure consistency.”
As discussed above, training was also a challenge. The technology was user-friendly, but not all staff members were comfortable with digital tools. AON found that in-person training was far more effective than virtual sessions. “Face-to-face builds confidence,” Rainey noted, “especially when you’re asking people to do something new.”
ven when the infrastructure was in place, patient engagement remained a hurdle. Many patients did not understand what PIN services were or why they mattered. “Some [patients] just don’t care,” Rainey said. “Others need more information to make an informed decision.” Her team focused on empowering staff to explain the value of these services and help patients see them as part of their health plan benefits.
Despite the obstacles, the early results have been promising. “We’re seeing the impact,” Rainey said. “And that’s what keeps us going.”
A Dedicated Resource Coordinator
At the heart of AON’s PIN rollout is a team member who may not always be visible to patients but is vital to their care—the resource coordinator. As Rainey described, the 1 mission of this full-time team member is to ensure that every patient in every market has access to the right community resources at the right time. “Her whole job is to vet and recommend resources in each individual market,” Rainey explained. “She researches, calls, confirms availability, checks for funding—everything.”
This behind-the-scenes work ensures that when a patient needs transportation, housing support, financial assistance, or food access, the care team is not scrambling. They already have a vetted list of reliable, up-to-date options. “She is a wonderful, wonderful, wonderful resource to us,” Rainey said. “And we’re so thankful to get to share that with our practices.” In a system where social needs can make or break a patient’s ability to complete treatment, this role is not just helpful—it’s essential.
Early Results and Future Opportunities
Since launching PIN services in early 2025, AON has already begun to see promising signs of impact. “We’re already seeing improvements in patient-reported outcomes,” Rainey noted. These early indicators suggest that addressing SDOH—such as transportation, housing, and financial stress—can lead to better engagement and potentially improved clinical outcomes. Looking ahead, AON sees several key opportunities to expand and enhance the program:
Despite the challenges of scaling a new program across a large and diverse network, Rainey remains optimistic. “We’re slightly ahead of schedule,” she said. “And we’re seeing real momentum. The more we learn, the more we can refine and expand.”
Rainey closed with a message that resonated across the room as she declared, “We’re already doing the work. Now we need to get paid for it, scale it, and make it sustainable. Because our patients deserve more than just treatment—they deserve whole-person care.”

Facilitators
Founded in 1971 in Baton Rouge, Mary Bird Perkins Cancer Center has grown into a comprehensive cancer care network with over 700 team members and 21 locations. The cancer center provides radiation and medical oncology care and mission-based services such as free cancer screenings, patient navigation, and financial assistance.
Making the Business Case
To make a compelling business case for developing a mobile cancer screening program, Renea Austin-Duffin advised that the first and most critical step is a thorough needs assessment. This assessment should answer the foundational questions of who, what, where, when, and why—with each informing the program’s design, funding strategy, and long-term sustainability. Below, Austin-Duffin shared the business case that Mary Bird Perkins Cancer Center has used for its Prevention on the Go mobile screening program.
The Who: Identifying the Target Population
Begin by defining the population most in need of early cancer detection services. This step includes analyzing demographic data to identify groups that are:
“[At Mary Bird Perkins], we serve the uninsured, the underinsured, the marginalized—those who would otherwise fall through the cracks,” Austin-Duffin explained. “Knowing who you serve allows you to tailor services and outreach strategies effectively.”
The What: Determining the Services to Offer
The needs assessment should also identify the most prevalent cancers in the region and the types of screenings that are most urgently needed. For example, in Louisiana, the top cancers include breast, prostate, colorectal, and skin cancer. Based on these data, Mary Bird Perkins designed a program that offers 5 types of screenings along with patient navigation, education, and follow-up care. The what also includes defining the program’s value proposition. For Mary Bird Perkins, Austin-Duffin explained, this includes:
The Where: Locating the Greatest Need
Geographic analysis is essential to determine where services are most needed. This step includes mapping cancer incidence and mortality rates, having access to primary care, and considering social determinants of health such as income, food insecurity, and transportation access. Austin-Duffin cited East Carroll Parish in Louisiana as a prime example—a rural area with a 51% obesity rate, 36% smoking rate, and a median household income of just $30,700. “It’s one of the poorest areas in the country,” she said. “And it’s exactly where we need to be.”
The When: Implementation Timeline
From a program development perspective, the timeline should include initial planning and stakeholder engagement, development of an operational budget, identification of funders and partnering organizations, and event coordination. (For a deeper dive on implementation, please see the section From Vision to Reality: An Implementation Roadmap, below.) Mary Bird Perkins’ Prevention on the Go program evolved over 2 decades, starting with community center screenings in 2002 and expanding to a fleet of 4 mobile clinics by 2025.
The Why: Making the Case for Investment
The why is the heart of the business case. It must clearly articulate the problem the program is solving and the impact the program will have. In Louisiana, the why was stark—high cancer mortality, poor health behaviors, and limited access to care. “We had people showing up with late-stage diagnoses,” Austin-Duffin said. “We had to do something.” The business case should include:
By answering the who, what, where, when, and why through a comprehensive needs assessment, a foundation is laid for an impactful and sustainable mobile screening program. As Austin-Duffin put it, “You can’t secure funding until you know what you’re going to do—and you can’t know what to do until you understand the need.”
Staffing and Equipping a Mobile Mission
The Prevention on the Go program is staffed by a core team of 11 full-time professionals who play critical roles in its day-to-day operations. At the helm is Austin-Duffin, who oversees the strategic direction and execution of the program. Supporting her are 2 regional directors who manage operations across the program’s expansive service area. The team also includes several regional managers responsible for a specific geographic zone. These managers coordinate logistics, build community relationships, and often serve as the face of the program in their regions. One of the regional managers also doubles as a mobile clinic driver, a testament to the team’s flexibility and hands-on approach.
Two licensed practical nurse (LPN) navigators are central to the program’s patient care model. These LPNs attend screening events, provide health education, and guide patients with abnormal findings through the often-complex process of follow-up diagnostics and treatment. Their work includes everything from scheduling appointments to arranging transportation and financial assistance. An outreach coordinator supports grassroots engagement, while a program coordinator manages logistics such as inventory, promotional materials, and patient reminders. Notably, the team also includes a dedicated marketing specialist who works exclusively on the program, ensuring that every event is well publicized and that community partners and sponsors receive appropriate recognition. “We’re an all-female team—except for Kyle [Bove], our marketing lead,” Austin-Duffin said proudly. “And we all pitch in. Whether it’s setting up tents or answering the hotline, everyone does what it takes.”
The program operates a fleet of mobile medical units affectionately named Early Bird I, II, and III; a fourth unit is on the way. These clinics are fully equipped to provide screenings for breast, prostate, colorectal, skin, and oral cavity cancers. Each unit includes examination rooms, refrigeration for biospecimens, and medical equipment tailored to the screenings offered.
The newer units are built on recreational vehicle–style chassis for improved reliability and maneuverability. The latest unit includes a mammography suite, allowing the program to offer breast cancer screenings independently for the first time. Each mobile clinic is supported by a rotating team of nurse practitioners (NPs) and, when needed, specialists such as dermatologists or otolaryngologists. These providers are paid hourly and reimbursed for travel and lodging when events take them outside their home cities.
In addition to the mobile clinics, the team uses 3 organizational vehicles for outreach and event support. These vehicles reduce mileage reimbursements and improve efficiency. Equipment includes tents, tables, chairs, laptops, tablets, and promotional materials that are managed and maintained by the team.
To streamline operations and enhance patient care, the program uses a custom-built electronic health record (EHR) called MyPogo (My Prevention on the Go). This cloud-based platform allows for real-time data entry, appointment scheduling, risk assessments, and outcome tracking. It also supports marketing analytics by capturing how patients heard about the program, helping the team refine outreach strategies.
Funding the Mission: How Prevention on the Go is Sustained
The success of the Prevention on the Go program lies not only in its clinical impact and its financial sustainability; built on a diverse and strategic funding model, the program is a case study of aligning mission-driven health care with sound fiscal management. From revenue generation to expense control, every dollar is accounted for to maximize community impact. The program’s revenue model is intentionally broad, ensuring resilience and flexibility. In fiscal year 2024, the program raised approximately $3 million—more than enough to cover its $1.8 million operating budget and reinvest in future growth:
Operating a mobile screening program like Prevention on the Go is resource-intensive, but every expense is carefully managed to ensure maximum return on investment as measured not in profit but in lives saved.
Of note, the operating budget does not include the cost of screenings, which varies by type (cost per screening: breast cancer, ≈$5000; prostate cancer, ≈$2500; skin cancer, ≈$2000). These costs include diagnostics, laboratory testing, advertising, and provider fees but exclude staff salaries and vehicle maintenance.
The Prevention on the Go program is committed to transparency and donor intent. “We cheer just as loudly for a $5000 grant as we do for a $2.3 million grant,” said Austin-Duffin. Every grant is tracked meticulously, and impact reports and budget-to-actual comparisons are provided to funders. This disciplined approach has earned the program a reputation for reliability and results.
The Power of People: Grassroots Advocacy and Community Partnerships
At the heart of the Prevention on the Go program is a simple but powerful truth: health care is most effective when it is rooted in the community it serves. While mobile clinics and clinical expertise are essential, the program’s true engine is its deep network of grassroots advocates, community outreach workers, and stakeholder partners who bring trust, credibility, and connection to every screening event.
In communities where access to health care is limited and mistrust of the medical system can run deep, grassroots advocacy is not just helpful, it’s essential. The Prevention on the Go team does not wait for people to come to them. Instead, team members go out into neighborhoods, walk the streets, visit local businesses, and engage residents in everyday places like grocery stores, barbershops, and churches.
“We do brightly colored flyers, but, more importantly, we have conversations,” said Austin-Duffin. “Our team members are out there talking to people, answering questions, and building relationships. That’s how we earn trust.”
These advocates are often the first point of contact for individuals who have never had a cancer screening. Their ability to connect on a personal level—sharing stories, listening to concerns, and offering reassurance—helps break down barriers and encourage participation.
The program’s outreach strategy is designed to meet people where they are literally and figuratively. Events are held in familiar, accessible locations—barbershops, community centers, places of worship, workplaces—and scheduled at convenient times, including evenings and weekends. This approach removes logistical barriers like transportation and time off work, making it easier for people to prioritize their health.
Signature events like the Barbershop Bash exemplify this strategy. Partnering with trusted local barbers creates a welcoming environment for Black men to receive prostate cancer screenings—an audience that is often underserved and at higher risk. “We had a line of men waiting before we even opened,” Austin-Duffin recalled. “That’s the power of going where people feel safe and respected.”
No organization can do this work alone. Prevention on the Go thrives because of its extensive network of partners, including:
These partners provide more than just logistical support—they lend credibility, amplify outreach, and help ensure continuity of care. For example, Federally Qualified Health Centers often refer patients to the program for screenings they do not offer in-house, whereas hos-pitals and diagnostic centers provide follow-up services for patients with abnormal results.
Partnerships are also key to sustainability. Many funders, including the United Health Foundation and local philanthropic organizations, support Prevention on the Go because of its demonstrated impact and collaborative model. “We show them the data, but we also tell them the patient stories,” Austin-Duffin said. “That’s what makes the case.”
In the end, the success of Prevention on the Go is not just about mobile units or medical equipment—it’s about people. It’s about the community members who spread the word, the partners who open their doors, and the team members who show up day after day with compassion and commitment. Together, they form a network of care that is as mobile, resilient, and rooted as the communities it serves.
Marketing With Purpose: Promoting Prevention on the Go
In a program as expansive and community-driven as Prevention on the Go, effective marketing is not just a support function—it’s a strategic pillar. With over 150 screening events held annually across Louisiana and Mississippi, the program relies on a robust, multi-channel marketing strategy to reach its diverse audiences. At the heart of this effort is a dedicated marketing specialist whose sole focus is to amplify the program’s visibility, engage communities, and ensure that every event is well attended and impactful. Kyle Bove holds this role and serves as the bridge between the outreach team and the broader marketing department.
“This program had grown so big that it needed someone fully dedicated to it,” Bove explained. “I work directly with Renea [Austin-Duffin] and Amanda [LaGrange] to make sure every event, every grant deliverable, and every outreach effort is supported with the right materials and messaging.”
Bove coordinates logistics and crafts the narrative. From designing flyers and infographics to managing social media campaigns and earned media opportunities, he ensures that Prevention on the Go’s voice is consistent, compelling, and community-centered. He also sits alongside the outreach team, not in the marketing department, to foster real-time collaboration and responsiveness.
The marketing strategy is both digital and grassroots. Online, the team leverages:
Offline, the program uses:
Each month, Bove produces a calendar of events and corresponding promotional materials. These are distributed by the outreach team during their community walks, when they engage residents face-to-face. “It’s old school, but it works,” Austin-Duffin said. “People respond to seeing a familiar face and a flyer they can hold in their hand.”
Marketing efforts are continuously refined through data collection. MyPogo includes a field asking participants how they heard about the event. This feedback loop allows the team to assess the effectiveness of different channels and adjust their strategies accordingly. For example, a recent pilot in the Delta region revealed that local newspapers and radio were more effective than digital ads in reaching rural residents.
Marketing also plays a crucial role in recognizing sponsors and partners. Logos are prominently featured on flyers, banners, and media appearances, providing visibility and value to those who support the program financially or in-kind. “We make sure our partners are seen and celebrated,” Bove noted. “It’s part of how we sustain these relationships.”
In short, the marketing strategy behind Prevention on the Go is as mobile, adaptive, and community-focused as the program itself. With a dedicated specialist at the helm, the team ensures that every screening event is not just a service—it is a story, a connection, and a call to action.
Inside the Events That Power the Program
At the core of the Prevention on the Go program are its events—vibrant, community-centered gatherings that bring cancer screenings, education, and support directly to the people who need them most. These events are more than just clinical encounters; they are moments of connection, empowerment, and hope. Each Prevention on the Go event is designed to be accessible, welcoming, and culturally responsive. The mobile clinics (the Early Birds) serve as the centerpiece of these events, providing screenings for breast, prostate, colorectal, skin, and oral cavity cancers. Patients are greeted by a compassionate team of nurse navigators, outreach coordinators, and clinical providers who guide them with dignity and care.
Among the most impactful are the program’s signature events, which combine health services with community celebration:
Education is a key component of every event. While patients wait for their screenings, nurse navigators provide information about cancer risks, screening guidelines, and healthy lifestyle choices. Infographics, recipe cards, and nutrition tips are distributed, often alongside bags of fresh produce donated by local grocers or farmers’ markets.
The events also serve as a platform for storytelling and advocacy. Patients who have benefited from Prevention on the Go often return to share their experiences, helping to build trust and encourage others to participate.
Each event is meticulously planned and evaluated. As discussed earlier, MyPogo is used to register participants, track outcomes, and collect feedback. These data not only inform future outreach strategies, they help secure ongoing funding. In 2024 alone, Prevention on the Go hosted 156 events, screened over 4200 individuals, and resulted in the diagnosis of 44 cancers—many of which may have otherwise gone undetected.
Growing Prevention on the Go
As Mary Bird Perkins Cancer Center reflects on more than 2 decades of impact through its Prevention on the Go program, the organization is not slowing down. Instead, it is accelerating with bold plans for expansion, innovation, and deeper community engagement. The vision is clear—to reach more people, detect more cancers early, and continue breaking down barriers to care 1 mobile clinic at a time.
One of the most immediate growth milestones is an additional mobile medical clinic, Early Bird IV. Like its predecessors, this unit will be fully equipped to deliver on-site cancer screenings, including mammography. It will also help alleviate the workload of Early Bird I, which has been on the road since 2006 and is nearing retirement. The new unit will allow the team to increase its presence in underserved regions, particularly in the Mississippi Delta and central Louisiana, where access to care remains limited.
“We’re not just replacing a vehicle—we’re expanding our capacity to serve,” said Austin-Duffin. “With 4 units, we can be in more places at once, and that means more lives saved.”
The program is also preparing to reintroduce cervical cancer screenings, which were previously discontinued due to challenges in securing follow-up care. This time, the approach will be different. The team plans to implement HPV self-collection kits and, for those who test positive, offer colposcopy services directly on the mobile unit. This innovative model will provide a full continuum of care for cervical cancer prevention, especially for uninsured and underinsured individuals. “We’ve got a doctor’s office on wheels,” Austin-Duffin said. “Why not use it to its fullest potential?”
Future plans also include expanding outreach to specific populations, including the LGBTQ+ community, firefighters, and younger women who are increasingly presenting with early signs of cancer. In 2025, the program will scale up its LGBTQ+ outreach events, building on the success of its inclusive screenings and culturally competent care. “We’ve integrated pronoun preferences into our patient records,” Austin-Duffin noted. “It’s about making everyone feel welcome.”
MyPogo will continue to evolve with enhancements that improve data collection, patient follow-up, and marketing analytics. The team is also exploring integration of telehealth consultations and digital education tools to extend their reach beyond physical events.
Sustainability remains a top priority. The team will continue to pursue diverse funding streams, including grants, corporate sponsorships, and community fundraising. They are also exploring the possibility of hiring a full-time NP to reduce reliance on contract providers and improve continuity of care. “We’re always thinking about what’s next,” said Amanda LaGrange, the program’s grants director. “Whether it’s a new funding opportunity or a new way to serve, we’re committed to growing smart and staying true to our mission.”


Launching a mobile cancer screening program like Prevention on the Go requires more than just a vehicle and a mission—it requires a strategic, step-by-step approach rooted in data, community engagement, and sustainable planning. For cancer programs looking to develop a similar program, Austin-Duffin shared this detailed playbook that guided Prevention on the Go from concept to execution, offering a replicable model for others.

Facilitators
Decentralized Clinical Trials: 101

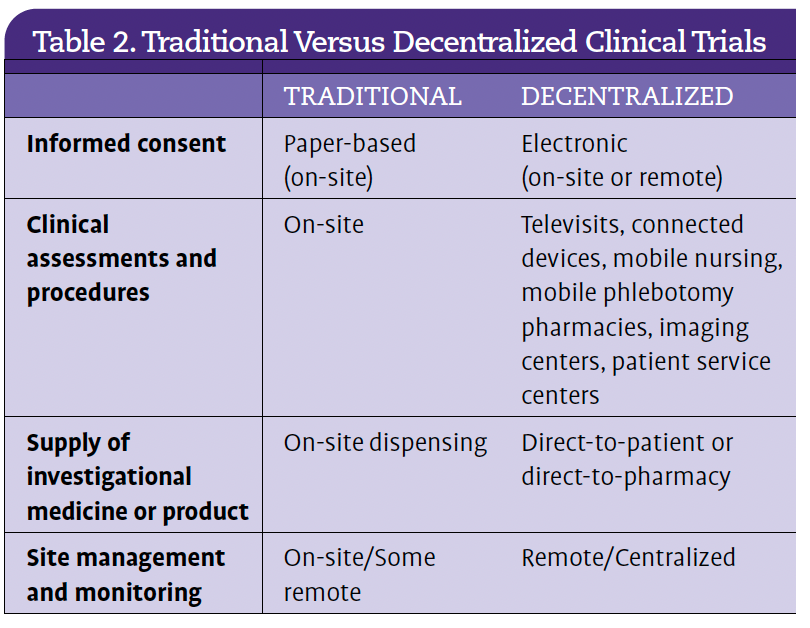
Decentralized clinical trials involve conducting trial-related activities outside of traditional research sites. This could mean using telemed-icine, home nursing, wearable devices, or local laboratories and pharmacies to collect data and deliver care. Decentralized clinical trials are not a novel concept. “The first decentralized elements were used as early as 2003,” noted Jane Myles, referencing early efforts by companies like Lilly and Pfizer. She referred to Pfizer’s REMOTE trial as one of the first fully decentralized clinical trials that allowed participants to enroll and participate without visiting a clinical site. Launched in 2011, it focused on overactive bladder and not cancer specifically, but it set the precedent for remote participation in clinical trials, including future applications in oncology. “These patients never saw an investigator,” Myles said. “And yet the FDA approved the design before the trial even began.” Table 2 is a comparison of traditional and decentralized clinical trials.
While decentralized clinical trials are not new—the way they are being combined—enabled by technology and a patient-first mindset is new. And the COVID-19 pandemic accelerated the adoption of decentralized methods, revealing both their feasibility and their necessity. Patients proved they were ready—even eager—to participate in trials from the comfort of their homes or local care centers.
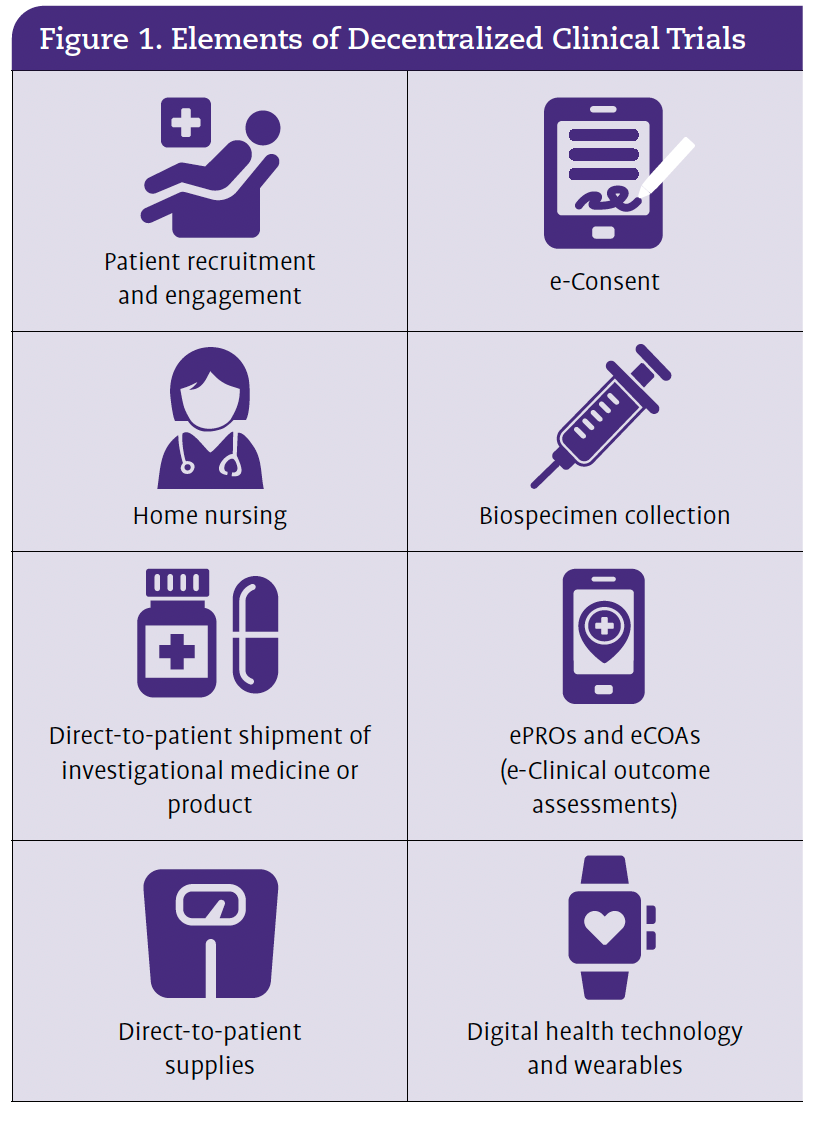
Regulators responded with guidance that supports these innovations, and sponsors began embedding decentralized clinical trial elements into protocol design from the outset (Figure 1). Still, after the pandemic, many health care organizations reverted to traditional models, and Myles urged meeting attendees not to let that momentum fade.

In oncology, patients often face high disease burdens and logistical challenges, and decentralized clinical trials offer a lifeline. “If you build the trial with these elements in mind and a really intentional, patient-focused approach, the patients want to do this,” Myles emphasized. Decentralized clinical trials can reduce travel, increase comfort, and allow patients to remain under the care of their trusted local providers. The benefits extend beyond convenience. According to Myles, decentralized clinical trials can improve recruitment, retention, and diversity. “We’re not just talking about race and gender,” she said. “We’re talking about regional diversity—reaching rural and remote patients who otherwise wouldn’t have access.”
Practical Strategies for Cancer Programs
For cancer programs considering decentralized clinical trials, Myles offered several actionable strategies:


Overcoming Barriers
Despite growing support, challenges remain. Regulatory ambiguity, global variability, and technological interoperability continue to slow adoption of decentralized clinical trials. But Myles is optimistic. “We have a lot of guidance now—from the US, Japan, Europe, and Canada. Regulators want these options to be available.”
She also challenged myths about patient readiness. “Many are already using FaceTime and telehealth. They’d be shocked that you didn’t make that option a possibility.”
As decentralized clinical trials become more viable, Myles believes the industry faces the moral question, “How can we deny access to individuals who require decentralized methods in order to participate?” For cancer programs, the answer is clear—embracing decentralized clinical trials is not just a technological upgrade; it’s a commitment to equity, inclusion, and patient-centered care.
A Blueprint for Decentralized Oncology Research
J. Caitlin Morrison of the UNC Lineberger Comprehensive Cancer Center laid out a practical, patient-centered roadmap for decentralizing clinical trials—particularly in oncology. Her message was clear—decentralization isn’t just possible, it’s essential for equitable access and sustainable research.
Morrison began by referencing the recent FDA guidance that distinguishes between complex investigational tasks (requiring specialized knowledge and confined to clinical trial sites) and routine clinical care, which can be performed anywhere.3 “Everything else,” she emphasized, “can happen in the community.” Morrison said that this regulatory clarity opened the door for a 3-tiered model of decentralization:
UNC’s research model focuses on the first 2 tiers, enabling broad participation without bureaucratic burden.
The model was born from necessity. “We had patients flying in from around the world for CAR T-cell therapy,” Morrison explained. “But these patients weren’t going to come back for 15 years of follow-up.” So, UNC developed remote monitoring systems, proving that patients could remain compliant and engaged from afar. “Over 95% of patients wanted to participate in remote procedures,” she noted. This hybrid model—in which patients receive initial treatment at UNC and long-term follow-up in their local communities—has now been applied to over 150 patients across 17 protocols.
Morrison has spent the past year touring North Carolina, meeting with local health care providers to offer education about participation in decentralized clinical trials. “Access to clinical trials is access to quality care,” Morrison said, echoing a sentiment she heard repeatedly. Participation offers 2 key benefits for providers. First, referring patients to decentralized trials helps maintain the American Cancer Society Commission on Cancer accreditation. Second, providers can bill (keep the income from) standard-of-care services they deliver to patients on clinical trials. An additional benefit is that participation does not exclude providers from authorship or study design. “Just because they’re not engaged in research doesn’t mean they can’t be on the publication,” Morrison clarified.
UNC’s decentralized clinical trial approach is designed around the patient. QR codes in exam rooms and after-visit summaries link to trial opportunities. In the past year alone, over 5000 patients and 200 providers accessed trial information through these codes.
Patient education materials were adapted to meet the needs of North Carolina’s diverse population, including those with second-grade reading levels. “We had to make it visual and simple,” Morrison explained.
Patients are remotely screened and consented, often with help from local providers using existing telehealth infrastructure. “Many clinics already had Zoom rooms for genetic counseling,” Morrison said. “We just repurposed them.”
Drug shipments are handled in-house. “Our coordinators pick up the pills, box them, and mail them,” Morrison explained. Patients return pill diaries via FedEx or through local clinics and libraries. Communication is bidirectional with emergency cards and clear protocols for reporting adverse events. Sample collection is similarly streamlined. Patients receive kits with picture instructions and arrange for blood draws at routine lab visits.
To ensure quality, UNC uses enhanced risk-based monitoring and tracks visit types and deviations. “We’re analyzing these data to improve the patient experience,” Morrison said. Electronic case report forms are tailored to capture visit locations and reasons for deviations whether due to patient convenience, travel issues, or compliance.
UNC’s success hinges on collaboration. Morrison credited local providers, community leaders, and her co-principal investigator, Dr. Carrie Lee. “We didn’t start with the protocol,” she said. “We started with the people.”
The results speak volumes: 22 patients enrolled in 1 year from just 1 trial, with 25 more protocols in the pipeline. Attendance at community meetings has surged, with even locum tenens physicians eager to participate.
Funded by the FDA, the project is part of a broader effort to reimagine clinical research. “The FDA was surprised oncology leaned into decentralized clinical trials during COVID—and then backed out,” Morrison said. “The FDA also couldn’t believe Form 1572 was seen as a barrier. Regulatory paperwork should never stand in the way of access.” With this model, Morrison and her team are proving that decentralized trials are not just a pandemic workaround—they are a path forward.
Morrison’s team is already looking ahead. Their HOPE (Hybrid Operations to Promote Equity) Tour has become a cornerstone of outreach, identifying local resources like transportation, food support, and flexible scheduling that enhance clinical trial participation. The model is also being applied to new studies, such as LCCC 2239, which is investigating radiation-induced cardiotoxicity. In this trial, local providers handle physical exams and imaging, while UNC manages consent, drug shipment, and oversight.
As Morrison concluded, “We’ve shown that strong partnerships with local health care providers make it possible to compliantly accrue and oversee patients. And we’re just getting started.”
How Mayo Clinic is Scaling Decentralized Research
Mayo Clinic’s Clinical Trials Beyond Walls initiative is built on the bold vision of creating a seamless, patient-centric, and equitable clinical trial experience. “We want to reach patients where they are,” Rebecca Kottschade said, “and empower them to participate in trials without the burden of geography, logistics, or technology.” As Kottschade, the program’s administrative leader, explained, “We’re not just enabling decentralized trials—we’re enabling decentralized capabilities across all trials, regardless of specialty.” To bring this vision to reality, Clinical Trials Beyond Walls developed 4 strategic objectives, each supported by concrete actions and measurable progress.
Optimizing the Experience
The first objective centers on improving the experience for both patients and study teams. “Clinical trials are complex,” Kottschade acknowledged. “It’s hard for patients to know what to expect, and it’s equally challenging for coordinators to manage all the moving parts.” To address this, Mayo Clinic established an Operations Enablement Team—clinical research experts who guide study teams through the adoption of decentralized tools like video visits and remote consent. These experts don’t just offer advice; they walk alongside teams, conducting discovery meetings, compliance reviews, and even dry runs to simulate workflows before patients are enrolled. One key innovation has been the use of electronic medication logs. Unlike traditional paper logs, which might not reach investigators until a patient’s next visit, these digital tools provide near real-time insights. “Now, a coordinator can call a patient and say, ‘I see you were nauseous after your dose today—how can we help?’” Kottschade said. This shift improves care and enhances data quality and responsiveness.
Expanding Access
The second objective is about breaking down barriers—geographic, financial, and logistical—that often prevent patients from participating in clinical trials. “We’re thinking about the person who lives 5 hours away from a research site,” Kottschade said. “They shouldn’t have to take a day off work or find childcare just to participate.” To that end, Clinical Trials Beyond Walls has implemented a suite of decentralized services, including remote biospecimen collection, video visits, and medication delivery. These services are designed with flexibility in mind, allowing patients to choose between in-person and remote participation based on their preferences and resources. Mayo Clinic has also centralized device services so study teams no longer have to source tablets or wearables on their own. “They just come to us and say, ‘I need a pulse ox (oximeter),’ and we take care of the rest,” Kottschade said.
Improving Inclusion
Inclusion is more than a buzzword for the Clinical Trials Beyond Walls team—it’s a guiding principle. Kottschade emphasized the importance of community engagement, noting that patients are more likely to participate when they trust their local providers and community leaders. “We’re asking, ‘What are the needs in your community, and how can we support them?’” she said. This approach has led to partnerships with local health care providers and the development of culturally sensitive educational materials. It has also informed the design of flexible protocols that accommodate diverse patient needs and preferences. Clinical Trials Beyond Walls has begun gathering data on patient preferences and barriers, using pilot studies to refine its approaches. The initiative emphasizes optionality, ensuring that patients can choose the method of participation that best suits their needs and circumstances.
Driving Adoption
Finally, the Clinical Trials Beyond Walls initiative is committed to making decentralized research easier for study teams to adopt. “For many teams, this is all new—the technology, the workflows, even the language,” Kottschade said. To support them, Clinical Trials Beyond Walls launched a consult service that offers everything from protocol design support to budgeting guidance and IRB navigation. (More detailed information on this consult service is available below.) The team has also created a tiered support model, ranging from self-service guides for tech-savvy teams to high-touch assistance for complex implementations. “We’re building a pyramid of customer service,” Kottschade explained, “so that no matter where a team is in their journey, we can meet them there.” The results speak for themselves. In 2024 alone, Mayo supported over 2500 active clinical trials across its 3 main campuses in Rochester, Minnesota; Phoenix, Arizona; and Jacksonville, Florida. Of those, 708 trials incorporated decentralized capabilities beyond remote consent, a clear indicator of the program’s rapid adoption and scalability. And as Kottschade noted, the demand is growing—not just for tools, but for the thoughtful, patient-centered infrastructure that Clinical Trials Beyond Walls is building.
Building Foundational Capabilities
Clinical Trials Beyond Walls has identified 6 foundational capabilities that support decentralized clinical trial participation:
Once again, these services are designed to be flexible. “Not every capability works for every trial or every patient,” Kottschade said. “Optionality is key.” For example, if a patient doesn’t have a smart-phone, they can still participate via phone calls. If they prefer in-person visits, that option remains.
Developing a Consult Service
As stated earlier, Clinical Trials Beyond Walls has built a robust consult service designed to guide study teams through the complexities of decentralized clinical trial implementation from protocol design to troubleshooting. Whether a team is launching a new investiga-tor-initiated trial or trying to rescue a struggling study, the consult team is available to assess needs and recommend decentralized solutions. “Sometimes a trial is in trouble,” Kottschade said. “We step in and ask, ‘Would a video visit help? Would remote phlebotomy make a difference?’” The consult service is staffed by a multidisci-plinary team with expertise in clinical research operations, digital product development, and regulatory compliance. This consult team provides:
Real-World Impact and National Reach
One of the key metrics the Clinical Trials Beyond Walls team is tracking is the percentage of patients enrolled from national zip codes, defined as areas located more than 120 miles from a Mayo Clinic site. These patients would traditionally face significant barriers to participation due to travel, time, and cost; they can now engage in clinical research from their homes or local communities. “We’re seeing more patients from rural and underserved areas participating in trials they never would have had access to before,” Kottschade noted. This shift improves equity and enhances the generalizability of trial results by including more diverse populations. The team has also observed improvements in patient retention and compliance. For example, electronic medication logs allow investigators to monitor adherence in near real-time. “If a patient logs nausea after a dose, the study team can follow up immediately,” Kottschade explained. “That kind of responsiveness improves both safety and engagement.”
The Future: Iteration and Partnership
Clinical Trials Beyond Walls is not a static program—it’s a dynamic, evolving model built on continuous learning and collaboration. As Kottschade emphasized, “We’re not just building a toolkit. We’re building a system that learns from itself and grows stronger with every trial.” At the heart of this future-focused approach is iteration. Clinical Trials Beyond Walls is actively funding and supporting pilot studies across various specialties to test decentralized capabilities in real-world settings. These pilots serve as living laboratories, allowing the team to identify operational barriers, assess patient experiences, and refine workflows. “We learn what works, what doesn’t, and we use that to improve the next trial,” explained Kottschade. This iterative process is supported by a multidisciplinary team of clinical researchers, digital product developers, and data scientists who analyze each use case to determine how data flow, where they should be stored, and how they integrate with systems like the EHR or electronic data capture platforms. “Understanding the data flow is one of the biggest challenges,” Kottschade noted. “But it’s also one of the most important pieces for scaling.”
Partnership is equally vital to the future of the program. Clinical Trials Beyond Walls is actively building relationships with local health care providers, community organizations, and regulatory bodies to extend the reach of clinical research. “We’re asking, ‘How can we bring the research infrastructure to the patient instead of asking the patient to come to us?’” Kottschade said. This includes working with local clinics to support decentralized clinical trial procedures, such as lab draws or medication administration, and ensuring that community providers have the tools and training needed to participate. It also involves engaging with regulators to clarify expectations and streamline approvals for decentralized methods.
Looking ahead, Clinical Trials Beyond Walls envisions a future in which decentralized capabilities are not just an option but a standard part of clinical trial design. For other institutions looking to replicate this success, the Mayo Clinic’s model offers a clear roadmap. Start with pilot studies, build a multidisciplinary support team, and prioritize both patient experience and operational excellence. The result is a research ecosystem that truly extends beyond walls—reaching more patients, generating better data, and ultimately delivering more cures.
Bringing Clinical Trials Home: The Sanford Health Model
Sanford Health, the largest nonprofit rural health care system in the US, spans a vast 200,000-square-mile region across the Dakotas, Minnesota, Iowa, and Montana. “It’s about the size of Texas,” Lora Black, RN, MPH, vice president of Clinical Research at Sanford Health, noted, emphasizing the logistical challenges patients face in accessing care. With 46 medical centers and 222 clinics, Sanford’s footprint is wide, but its commitment to patient-centered research runs even deeper. Sanford Health’s journey toward decentralized clinical trials began over 15 years ago with a single physician—its only gynecologic oncologist at the time—who questioned why clinical trials couldn’t be conducted remotely. “She was a research champion,” Black recalled. “She petitioned HHS [the US Department of Health and Human Services] and the cooperative groups to try telemedi-cine-based trials. And she succeeded.”
What began as a telemedicine experiment has evolved into a robust decentralized clinical trials program. The rationale was clear. Geography, transportation, financial burden, and caregiver responsibilities were significant barriers to trial participation. “We knew we had to bring trials closer to home,” Black said.
The impact has been profound. From the first enrollment in 2014 to 2023, Sanford’s decentralized clinical trials initiative, operationalized between Sioux Falls, South Dakota and Fargo, South Dakota, saved patients and caregivers an estimated 689 hours annually—time that would have otherwise been spent traveling from Fargo to Sioux Falls, for study visits. In reviewing historical data, an average of 26.5 telemedicine visits per year across the program reduced approximate patient travel time by 185.5 hours and and more than 150 patient hours on site for visits and treatment.
While 24 enrollments over a decade may seem modest, Black urged the audience to consider the broader implications. “That’s 1 physician, 1 specialty, 1 organization,” she said. “Imagine the potential if we scale this.”
Sanford is now looking ahead. With the 2024 FDA guidance and industry momentum supporting decentralized models, the organization is developing tools to integrate decentralized clinical trials into routine practice. This includes matching study requirements with site capabilities and patient locations and ensuring access to labs, imaging, pharmacy, and infusion services.
“We’re building a framework to make decentralized clinical trials sustainable,” Black explained. “We want to measure impact, demonstrate return on investment, and secure sponsor support. Most importantly, we want to make research accessible to every patient, no matter where they live.” Black’s presentation resonated with a powerful message: decentralization isn’t just a strategy—it’s a commitment to equity in health care. “Location should never be the reason someone can’t access a clinical trial,” she concluded.
Lilly’s Vision for Expanding Access to Clinical Trial
“Only 7% of US cancer patients participate in clinical trials,” said Brad Kleinschmidt, a senior director at Lilly. “That means 93% are left out—and we’re determined to change that.” Kleinschmidt, along-side colleague Melissa Jacanin, outlined Lilly’s bold initiative to expand access to oncology clinical trials across the US—not just for Lilly-sponsored studies, but for all. “This isn’t about our trials,” Jacanin emphasized. “It’s about making sure the patients who will ultimately use these medicines are represented in the data that support them.”
Lilly’s strategy is built on 2 pillars: environment shaping and operational enablement. Environment shaping focuses on shifting public and professional perceptions of clinical trials. One campaign, for example, asks providers to consider, “If it were you, wouldn’t you want to hear about clinical trials?” This is a powerful nudge toward normalizing trial conversations at diagnosis.
Lilly is taking a multifaceted approach to enabling decentralized clinical trials. One of the company’s key strategies involves rethinking how clinical trial protocols are designed. For instance, Lilly has begun bundling multiple trials into a single protocol when they target similar patient populations. This bundling reduces the administrative burden on sites and increases the likelihood of patient eligibility. In another example, Lilly now allows patients to receive 1 cycle of standard-of-care treatment before officially enrolling in a trial. This additional time gives patients and providers more time to build trust and make informed decisions.
Technology plays a central role in Lilly’s efforts. The company is piloting artificial intelligence (AI) tools that can prescreen patients across multiple sites, identifying only those patients most likely to be eligible. In 1 pilot, a data integration platform aggregates information from 36 community locations—many of which use different EHRs—giving central coordinators a unified view of potential participants. Jacanin, who leads innovation efforts at Lilly, shared her enthusiasm for AI-powered pre-screening tools that can identify eligible patients more efficiently. “Let the machines do the boring stuff,” she said. “That way, coordinators can focus on what matters—connecting with patients.”
Lilly is also embracing decentralized trial elements such as eConsent, video visits, remote patient monitoring, and home-based services like phlebotomy and nursing. Lilly supports shipment of oral investigational products directly to patients or local providers, with compliance supported through tools like pill diaries and video check-ins.
To reduce barriers for both patients and trial sites, Lilly is covering investigational treatments and, in some cases, the full cost of standard-of-care treatments. Lilly also offers flexibility in vendor use, allowing sites to use their own systems if they meet compliance standards rather than mandating Lilly’s preferred vendors.
Recognizing the importance of site readiness, Lilly encourages research sites to develop and document standard operating procedures for decentralized clinical trial processes. This transparency helps the company approve decentralized methods more quickly and confidently. Additionally, Lilly provides training and support to ensure that principal investigators can maintain oversight, even when trial activities are conducted remotely.
Through these efforts, Lilly is expanding access to clinical trials and helping to reshape the clinical research landscape to be more inclusive, efficient, and patient-friendly.
The team’s message was clear—decentralization is not just a technological shift but a moral imperative. “With regulatory clarity and operational confidence,” Kleinschmidt concluded, “we must ask ourselves, ‘How can we deny access to those who need decentralized methods to participate?’”


Facilitators:
How Data Can Empower Providers in Payer Negotiations

In a health care landscape often dominated by payer influence, Matt Mulherin delivered the powerful message that providers are not powerless. In fact, with the right data and mindset, providers can transform payer relationships from adversarial standoffs into account-able partnerships. “Too often, it feels like payers hold all the cards,” Mulherin began. “They have the resources, the leverage, and the ability to dictate terms. But that’s only part of the story.” He acknowl-edged the imbalance but emphasized that providers have untapped power—especially in their data.
Mulherin urged providers to stop accepting payer terms at face value and instead use contract intelligence to hold payers accountable. “But you can’t hold someone accountable for paying you correctly if you don’t know what you’re supposed to be paid,” he said. That means understanding every Current Procedural Terminology (CPT) code, every fee schedule, and every contractual term—no small feat, but a necessary one.
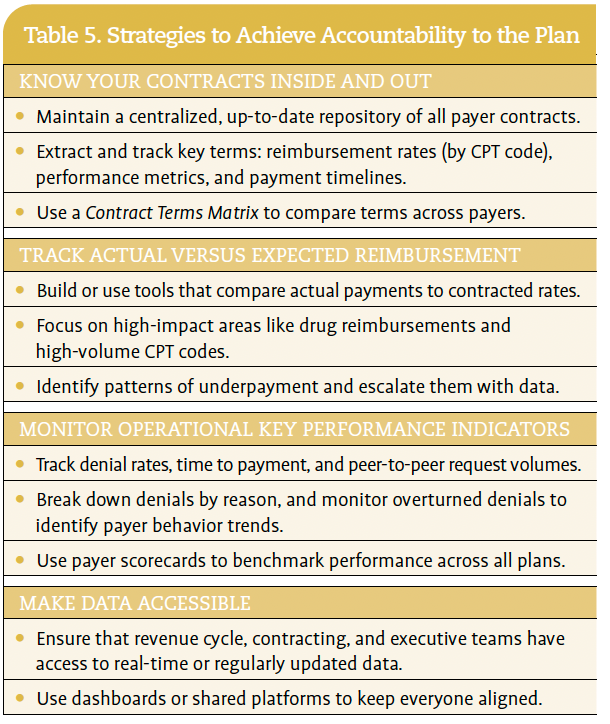
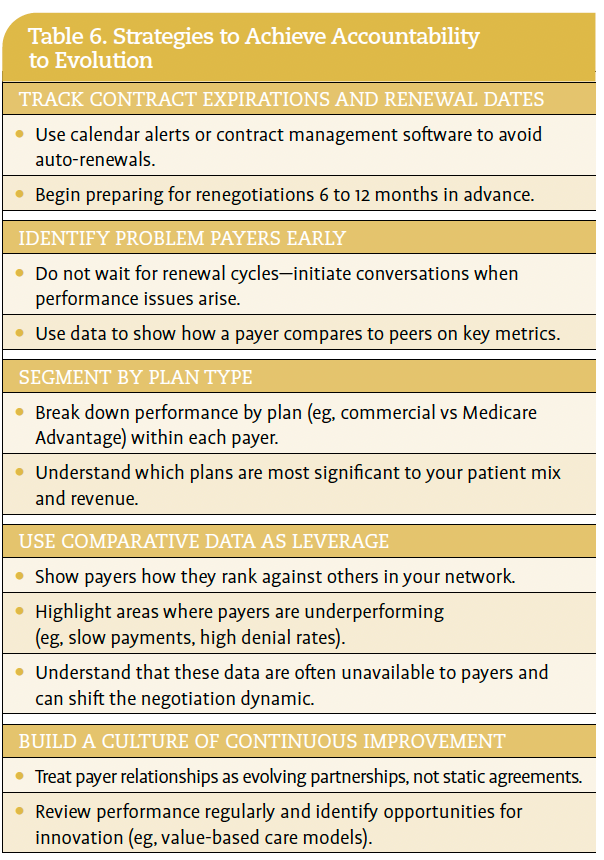
Building Accountable Partnerships
Mulherin outlined 2 pillars of building accountable partnerships: accountability to the plan (Table 5) and accountability to evolution (Table 6). The first ensures that payers adhere to existing contract terms, including reimbursement rates and performance metrics like denial rates and time to payment. The second focuses on using data to drive improvements and renegotiations, especially when contracts are up for renewal or payer performance falls short.

Internal Alignment
Mulherin also stressed the importance of internal alignment. Having the right data is only part of the equation—ensuring that the right people have access to it and use it consistently is what turns information into impact. Mulherin’s cancer program made a deliberate effort to break down silos between departments. Revenue cycle teams, payer contracting staff, and executive leadership were all given access to the same centralized data repository. This meant that everyone—from billing to the boardroom—worked from a shared understanding of payer performance, contract terms, and financial goals.
This alignment had several tangible benefits. For one, it enabled faster, more confident decision-making. When a payer issue arose, there was no need to chase down spreadsheets or reconcile conflicting reports. Everyone could see the same scorecards, the same reimbursement benchmarks, and the same contract timelines.
It also fostered a culture of accountability. With clear visibility into how each payer was performing—and how that performance affected the organization—teams were more proactive in flagging issues and proposing solutions. Contracting staff could approach negotiations with real-time insights, while revenue cycle teams could prioritize claims follow-up based on payer behavior patterns.
Moreover, internal alignment helped the organization stay agile. When a contract was nearing renewal or a payer’s performance began to slip, the team could mobilize quickly. The team was not reacting in isolation—it was responding as a coordinated unit, with shared goals and a unified strategy. In essence, internal alignment turned data into a strategic asset. It ensured that every part of the organization was rowing in the same direction, making it possible to hold payers accountable with clarity, confidence, and cohesion.
Real World Impact
Mulherin shared real-world examples of the impact this approach can have. His team reclaimed $375,000 through targeted payer projects. This included $37,000 in individual claim errors, meaning a single payer made a mistake on a batch of claims that was caught and corrected thanks to detailed claims analysis; $50,000 from improper onboarding that led to billing issues for 1 physician; and $40,000 from systematic errors in how the practice management system calculated reimbursements, which was also uncovered and corrected.
Most impressive, by comparing actual payments to contracted rates—especially high-cost items like oncology drugs—Mulherin’s team identified and reclaimed half a million dollars in underpayments. These were recovered either through individual claim corrections or broader payer projects. For other cancer programs seeking a similar comparison, Mulherin advised a high-dollar, high-frequency focus. Rather than reviewing every claim, his team prioritized high-dollar items (eg, chemotherapy drugs) and low-dollar but high-frequency CPT codes (eg, procedures billed thousands of times per month).
“These aren’t just numbers,” he said. “They’re proof that when you track performance and compare it to expectations, you can recover real value.”
Additional benefits to the cancer program included:
Providers Have Power
One of the most compelling parts of his talk was the emphasis on mindset. “You are needed,” Mulherin reminded the audience. “Payers can’t afford to lose access to respected providers in the community.” By coming to the table with data—especially data that payers do not have—providers can shift the dynamic. “It changes the conversation. It gives you credibility and leverage.”
While it may feel like payers hold all the cards with their vast resources and national reach, Mulherin emphasized that providers bring equal value to the table—patients, community trust, and local market insight. “They need you as much as you need them,” he reminded the audience. “Especially if you’re a well-known, well-respected provider in your community.”
One of the most powerful tools providers have is their access to localized, real-time data—something payers typically lack. While payers may have national benchmarks and internal metrics, they often do not have visibility into how they perform within a specific market or against their competitors in that region. When providers come to the table with payer scorecards, denial rate comparisons, and reimbursement benchmarks, they shift the dynamic. “It changes the conversation,” Mulherin said. “You’re no longer just asking for better terms—you’re showing why they’re justified.”
This data-driven approach also gives providers the ability to challenge underperformance. If a payer’s denial rate is significantly higher than others, or if their time to payment is lagging, providers can present that evidence and demand improvement. And because payers care about their reputation and competitive standing, this kind of transparency can be a powerful motivator for change.
Moreover, providers can use contract expiration dates and renewal cycles as strategic leverage points. By tracking these timelines and preparing well in advance, providers can avoid auto-renewals of outdated or unfavorable contracts and negotiate from a position of strength.
Ultimately, the power that providers have in payer negotiations comes down to preparation, confidence, and clarity. As Mulherin put it, “You don’t have to accept the terms you’re given. You can—and should—bring your own expectations to the table.” With the right data and mindset, providers can transform payer relationships from 1-sided arrangements into true partnerships built on accountability and mutual respect. Mulherin’s message was clear: providers have more power than they think.
Texas Takes the Lead on PBM Reform
Dr. Chris Prakash shared that pharmacy benefit managers (PBMs) are a major barrier to affordable, accessible cancer care—and it’s time for reform. As a medical oncologist with Texas Oncology, Dr. Prakash sees firsthand how PBM practices disproportionately affect rural patients. “These patients are already traveling long distances and facing socioeconomic hardships,” he explained. “PBM policies only make it harder for them to get the care they need.”
PBMs act as intermediaries between health plans, drug manufacturers, and pharmacies; they have long operated in the shadows of the health care system. But as Dr. Prakash pointed out, their influence is massive. “Three PBMs—Caremark, Optum, and Express Scripts—control 80% of the national market,” he said. “They dictate formularies, steer prescriptions to affiliated pharmacies, and rake in billions through opaque pricing practices.”
The consequences are severe. Patients face higher out-of-pocket costs due to co-pay accumulators and spread pricing. Independent pharmacies, especially in rural areas, are being squeezed out by low reimbursements and post-pay clawbacks. “About 25% of rural pharmacies have shut down,” Dr. Prakash noted. “That’s not just a statistic—it’s a crisis.”
But Texas is fighting back. Since 2017, the state has passed a series of laws aimed at curbing PBM abuses. These include:
Dr. Prakash emphasized that these reforms did not happen overnight. “The turning point came in 2019, when legislators started hearing directly from patients and providers,” he said. “They began to under-stand the vertical integration between health plans, PBMs, and pharmacies—and how it was hurting people.”
One major hurdle remains: the Employee Retirement Income Security Act of 1974 (ERISA), the federal law that exempts many employer-sponsored health plans from state regulation. While the Supreme Court’s decision in Rutledge v Pharmaceutical Care Management Association (2020) opened the door for states to regulate PBMs, Texas laws have yet to fully incorporate ERISA plans. However, a recent opinion from the Texas Attorney General supports the state’s authority to enforce these laws—a promising development for future reform.
For states aiming to replicate Texas’s legislative progress on PBM reform, Dr. Prakash offered these clear, practical steps:
Build a coalition of stakeholders
Educate legislators
Advocate on the local, state, and national level
Work with stakeholders to draft targeted legislation that focuses on specific, actionable reforms
Looking ahead, Dr. Prakash outlined ongoing efforts to eliminate PBM self-dealing in Medicaid, increase audit requirements, and prohibit non-medical switching. “We’re not done yet,” he said. “But Texas has created a blueprint that other states—and maybe even the federal government—can follow.”
His final message to meeting attendees was that advocacy matters. “We need to keep showing up, keep sharing our stories, and keep pushing for change,” he urged. “Because, at the end of the day, this is about our patients—and they deserve better.”
A Centralized Pharmacy Model Improves Prior Authorization
At the Orlando Health Cancer Institute, a persistent challenge that undermined the efficiency of oncology clinics and delaying patient care was the cumbersome process of medication prior authorizations. “Our nurses were constantly on the phone, and our physicians were stuck arguing with insurance companies instead of focusing on patient care,” shared senior pharmacy director Andrea Ledford. “It was frustrating for everyone.”
To solve this challenge, Ledford launched a pilot program in 2023 to centralize the prior authorization process. A dedicated team of 2 full-time pharmacy technicians were tasked with managing all prior authorizations—both prospective and retrospective—for 28 oncology clinics, which later expanded to 36 clinics. The goal was to reduce clinic inefficiencies, alleviate physician workload, and improve patient access to timely treatment.
The implementation strategy was methodical and data-driven. The team began by mapping out the existing workflow and identifying bottlenecks. The new process required a shift from a reactive, retrospective model to a proactive, prospective one. In the old system, prescriptions were sent to retail pharmacies, which then initiated the prior authorization process—often by fax—leading to delays of several days. In contrast, the prospective model integrated directly with the electronic health record (EHR). Before a prescription left the cancer center, pharmacy technicians completed the prior authorization using automated prompts within the EHR. “Usually, the authorization comes back within 24 hours,” Ledford noted, “and then we can release the prescription to the destination pharmacy with the authorization already attached.”
To support this shift, pharmacy technicians were trained extensively on EHR navigation, including how to locate ICD-10 and CPT codes and extract relevant clinical documentation. Pharmacy technicians were granted expanded access and equipped with Adobe PDF tools to streamline form completion. “We taught them where to look for the information in the EHR,” Ledford said. “Then we created a structured communication process so that we didn’t have to call each other every 5 minutes.”
Secure messaging systems replaced phone calls, and a standardized workflow was developed to ensure consistency. Initially, some nurses were reluctant to give up control of the prior authorization process; through relationship-building and transparency, however, the transition was successful. Pharmacy technicians began their roles by rounding in clinics and meeting staff face-to-face. After 6 months, they were allowed to work remotely—a strategy that helped retain talent. “I haven’t had any turnover in about 18 months,” Ledford said.
The centralized pharmacy team also adapted to evolving payer requirements. As some insurers moved away from platforms like CoverMyMeds and developed their own portals, the pharmacy team took on the responsibility of managing these systems. This relieved clinic staff from having to learn and navigate multiple platforms. “I can’t imagine what the nurses would be going through if we hadn’t made the change,” Ledford admitted.
The results of the pilot were impressive. The approval rates for medication authorizations for the centralized pharmacy team and the traditional clinic-based model, respectively, were 97.4% and 93.5% (P = .00001). The difference was significant, but the benefits extended far beyond the numbers. Clinics reported improved efficiency, reduced patient wait times, and enhanced communication between departments. “We didn’t just improve metrics—we improved morale,” Ledford noted.
For providers, the impact was immediate and profound. Physicians were no longer pulled away from patient care to handle insurance paperwork. “I wanted therapy plans that facilitate care and bundle everything so it’s a minimum of 8 clicks to get a drug ordered,” Ledford said. “I don’t want our physicians stuck on the phone arguing why a patient needs Taxol-Carbo (paclitaxel-carboplatin) for lung cancer.” Nurses, once overwhelmed by phone calls and faxes, were freed to focus on clinical care. The reduction in administrative burden also helped stabilize staffing. “After COVID, many seasoned oncology nurses retired,” Ledford explained. “This program helped reduce burnout and turnover by removing one of the most frustrating parts of their job.”
For patients, the benefits were equally significant. Delays in treatment due to prior authorization bottlenecks were reduced, and anxiety levels dropped as access to life-saving medications became more predictable. “Patients were waiting in rooms longer, because staff were stuck on the phone,” Ledford recalled. “Now, they’re getting their medications faster and with fewer complications.” The centralized prior authorization team also took over troubleshooting when prescriptions were delayed, calling payers directly and navigating complex portals—tasks that previously fell to already overburdened clinic staff.
Looking ahead, Orlando Cancer Institute is expanding its program by integrating clinical pharmacists into the peer-to-peer and appeals process. “We’re creating structured notes to track outcomes of these interactions,” Ledford said, “so we can run reports and get metrics on what’s being accepted or denied.”
For other cancer programs considering a similar initiative, Ledford offered several practical tips:
Ultimately, Orlando Health’s centralized prior authorization model did not just streamline a process—it transformed the culture of care. “The patients are the ones who really benefited,” Ledford concluded. “And that’s what matters most.”
How Advocacy is Reshaping Cancer Care in Minnesota
In rural Minnesota, Dr. Wade Swenson, a medical oncologist at Lakewood Health System, has made legislative advocacy a core part of his practice. “We have a story to tell,” he said. “And our patients deserve to have their voices heard.” Dr. Swenson is proving that a small community of roughly 3000 people can drive policy change.
For cancer providers, advocacy is not just a professional responsibility—it’s a moral imperative. “When I’m in clinic, I’m focused on the patient in front of me,” Swenson said. “But when I’m at the state capitol, I’m fighting for all of them.”
Dr. Swenson’s advocacy focuses on payer-related barriers, including prior authorization delays, co-pay accumulators, fertility preservation, and telehealth restrictions (Table 7). In a local study, his team tracked prior authorizations over 3 months and found that while 100% were eventually approved, treatment delays ranged from 1 to 13 days. “Thirteen days might not sound like much,” he noted, “but for a patient with small cell lung cancer, that’s critical time lost.” Quantifying the impact on patient care helps make a compelling case for policy reform.

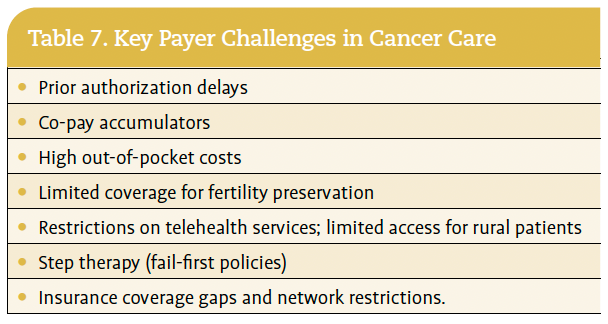
One of Dr. Swenson’s most impactful strategies has been involving patients directly in the advocacy process. In 2 cases, patients joined peer-to-peer calls with insurers. “It was eye-opening,” he said. “If they’re truly my peer, they should be talking to the patient too.”
Dr. Swenson also collaborates with groups like the Minnesota Society of Clinical Oncology and fertility advocacy organizations to amplify diverse perspectives to state and federal legislators. “These coalitions can be incredibly effective,” he said.
Dr. Swenson’s efforts contributed to Minnesota’s recent legislative win—a bill limiting prior authorization for chronic conditions and prohibiting it for preventive services and certain cancer treatments (Table 8.) His advice to other cancer programs? “Track your data, tell your stories, and build coalitions. Advocacy isn’t just policy—it’s patient care.”

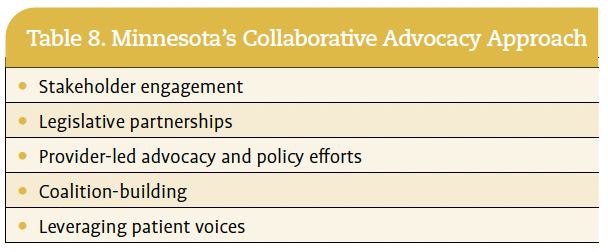
Implementing Subcutaneous Cancer Therapy
In a health care landscape burdened by rising costs, workforce short-ages, and increasing patient complexity, Dr. Raghava Induru, a medical oncologist and operations director at Atrium Health Levine Cancer, is championing subcutaneous drug delivery, which he said “could offer a path to better access, reduced operational strain, and improved patient experience—especially in community and rural settings.”
Dr. Induru illustrated the promise of subcutaneous therapy through 2 real-world patient case studies. One involved a patient with breast cancer who developed complications from an IV port, making subcutaneous trastuzumab-pertuzumab a more viable long-term option. Another case featured a rural patient with multiple myeloma—a business owner and father of 5—who needed flexible scheduling and preferred to avoid a port. Subcutaneous daratumumab allowed him to continue working while receiving care. “These are real-life [treatment] decisions shaped by more than just clinical data,” Dr. Induru emphasized.
The clinical evidence is compelling. Studies show that subcutaneous formulations of drugs like trastuzumab, rituximab, daratumumab, and nivolumab are noninferior to their IV counterparts in efficacy and safety. Patients overwhelmingly prefer subcutaneous administration due to shorter treatment times, less invasive procedures, and greater convenience. From an operational standpoint, delivery reduces chair time, optimizes staffing, and alleviates pharmacy preparation bottlenecks. “As a director of operations, I now understand how every minute in the infusion chair impacts the entire system,” Dr. Induru said.
However, transitioning to subcutaneous therapy is not without challenges. Payers often resist coverage, sometimes approving only limited doses or requiring repeated authorizations. “We’re seeing pushback even for well-established subcutaneous drugs,” noted an audience member from Jefferson Health. Dr. Induru acknowledged these barriers, emphasizing that solutions require collaboration across manufacturers, payers, providers, and health systems. “This is a new frontier,” he said. “We need to work together to make it viable.”
For cancer programs seeking to implement subcutaneous therapy, Dr. Induru offered these practical strategies:
Ultimately, Dr. Induru believes subcutaneous therapy represents a natural evolution in cancer care—one that aligns with modern expec-tations for convenience, efficiency, and patient-centeredness. “We’re not there yet,” he said, “but with the right planning and partnerships, we can get there—and our patients will be better for it.”
Monique J. Marino is senior director of editorial content and strategy at the Association of Cancer Care Centers in Rockville, Maryland.
References