Widely considered to be the fourth pillar of cancer management, immuno-oncology (I-O) has played an increasingly important role in cancer treatment. Broadly defined as the harnessing of the immune system to direct a response towards tumors, I-O therapy is a diverse field that encompasses cancer vaccines, monoclonal antibodies (notably, checkpoint inhibitors), adoptive cell therapies, oncolytic virus therapies, and non-specific immunotherapies (e.g., cytokines)
Beginning with the approval of the first checkpoint inhibitor (ipilimumab) in 2011 for malignant melanoma, rapid advances in I-O checkpoint inhibitor therapy have led to tremendous, well-tolerated, and durable clinical benefit in a number of patients with a variety of malignancies.1,2 Over the last five or more years, checkpoint inhibitors have been approved for more than 15 indications and this number is only expected to increase.3
To date, six checkpoint inhibitors have been approved including CTLA-4 (cytotoxic T-lymphocyte-associated protein 4) inhibitor (ipilimumab), programmed cell death protein (PD-1) inhibitors (nivolumab, pembrolizumab), and programmed death ligand-1 (PD-L1) inhibitors (atezolizumab, avelumab, and durvalumab).4
An estimated 1.6 million Americans will receive a diagnosis of cancer in 2017.5 Yet, despite 70% of people in the U.S. expressing a willingness to consider participating in a cancer clinical trial if asked to do so, less than 5% of adult patients with cancer who are eligible for clinical trials participate.6
Between 2006 and 2014, the number of clinical trials registered on ClinicalTrials.gov increased from 9,321 to 18,400.7 Immuno-Oncology trials have been no exception to this expansion. According to the “Medicines in Development for Immuno-Oncology 2017 Report,” from PhRMA in partnership with the American Cancer Society Action Network (ASCAN), more than 248 new I-O therapies and vaccines are currently in clinical trials or awaiting U.S. Food and Drug Administration (FDA) review.8
In addition, from 2015 to 2017, the number of combination studies listed on ClinicalTrials.gov combining PD-1 or PD-L1 inhibitors with other therapies has surged, growing from 215 to 765 (combination trials with pembrolizumab [n=268]; nivolumab [n=242]; durvalumab [n=123]; atezolizumab [n=83]; avelumab [n=18]; and others [n=49]).9
This article provides a brief overview of how clinical trial development is evolving to better reflect novel aspects of I-O therapies, with a nod to some logistical issues patients/families encounter with clinical trial participation. Over the last few years, checkpoint inhibitors have dominated the I-O landscape; thus, much of the article is focused on these agents. However, issues encountered with checkpoint inhibitor therapy clinical trials may be relevant to those encountered with other classes of I-O therapies in the future.
Clinical drug/biologics development is a long, complex, and costly process. In general, a new drug/biologic spends an average of 6.9 years in the clinical research phase, followed by an additional 10 months under FDA standard review.10,11 Many of the recently approved oncology agents, including checkpoint inhibitors, have been granted FDA designations that can shave significant time off the development/approval process (Table 1). In 2016, the median total priority review/approval time for drugs/biologics was 8 months after submission; however, this time in review can be much less. For instance, the total time to accelerated approval for atezolizumab was just over four months.11,12
Table 1.FDA Terminology
Source: fda.gov/ForPatients/Approvals/Fast/default.htm
While estimates vary widely, the average total cost of developing and bringing a new drug to market ranges from $161 million to $2 billion.13 A key component of this total cost is clinical trials. Top funders of clinical trials include the National Institutes of Health (NIH) and the pharmaceutical industry. Additional sources of funding include other U.S. federal agencies, universities, organizations, non-U.S. governmental agencies, and other non-U.S. sources. However, since 2006, the sources of funding for trials registered in ClinicalTrials.gov have been shifting (Table 2).7
Table 2. Funding Sources for All Trials Registered in ClinicalTrials.gov Between 2006 and 20147 Year of trial start Total number of registered trials Funding agency n (%) NIH Industry Other U.S. federal agency All Others 2006 9321 1376 (14.8%) 4585 (49.2%) 263 (2.8%) 3240 (34.8%) 2014 18400 1048 (5.7%) 6550 (35.6%) 339 (1.8%) 10597 (57.6%)
Analyses show that the total cost for one oncology study in the U.S. approaches $79 million, with an average per-patient cost of $59,500.13,14 Despite this significant financial investment, the dramatic clinical results seen with I-O agents has spurred alliances, investments, and research (Table 3).
Table 3.Snapshot of Advances in Cancer Immunotherapy Development8,15
The rapid clinical development and approval of I-O therapies reflects the frequent utilization of innovative adaptive trial designs that 1) enroll large numbers of patients early on, 2) use expansion cohorts, 3) analyze subsets of patients, and 4) work closely with the FDA through the accelerated approval process.2 Accelerated approval is based on data from surrogate or intermediate endpoints that strongly and reasonably predict clinical benefit, with the requirement that further confirmatory clinical data will verify actual benefit.16 Challenges with this approach can include questions such as what is the optimal duration of treatment, length of follow-up, and dosing modifications.16
To more fully recognize the clinical benefit seen with I-O therapy, approaches for assessing treatment response have needed to evolve. The scope of this evolution spans across multiple domains, including, but not limited to: developing new clinically meaningful endpoints and metrics, identifying robust biomarkers, and revisiting eligibility criteria. Further, many I-O studies are large in size and international in scope, making effective and efficient communication between stakeholders about trial modifications, management of atypical responses, and identification and management of immune-related adverse events challenging. Ensuring that well-defined master protocols, communication strategies, and management algorithms are in place can help offset these challenges.2
In the past, cancer clinical trials generally enrolled patients based on tumor histology and clinical characteristics and were primarily focused on incremental gains in traditional endpoints including: overall survival (OS), objective response rates (ORR), progression-free survival (PFS), disease-free survival (DFS), and patient-reported outcomes (PRO) of improvement or deterioration as endpoints, all balanced against toxicity.2,16,17
The mechanisms of action of I-O therapies are profoundly different compared with chemotherapy and targeted therapies. I-O medications target the immune system as opposed to directly targeting the tumor; in essence, the immune and anti-tumor response to I-O therapy is dynamic.16 For example, checkpoint inhibitor therapy has been associated with unique delayed kinetics of clinical response and atypical response patterns compared with cytotoxic chemotherapy or targeted therapy.2
This stresses the importance of incorporating additional clinically meaningful endpoints into trial design that more accurately reflect the biology of immunotherapies and more effectively capture the non-proportional and time-dependent treatment effects compared with traditional therapy (Table 4).2,16,17 Given the significant improvements seen in duration of response in some patients treated with I-O, quality of life (QoL) continues to emerge as an increasingly important endpoint.18
In addition, statistical analysis and modeling approaches for I-O clinical trial data may need to be refined to accurately reflect treatment effects seen with I-O agents (e.g., describing hazard ratios as a function of time and recognizing the impact of delayed separation of Kaplan-Meier curves).16,19
Lastly, the use of traditional metrics to assess treatment response (e.g., RECIST1.1, World Health Organization) may underestimate the clinical benefits of checkpoint inhibitor treatment.16 Use of modified response criteria to assess response to checkpoint inhibitor therapy makes allowances for these unique response patterns and allows for continued treatment in the face of apparent, clinically insignificant, disease progression.2
To date, a variety of modified response criteria have been used across I-O trials (e.g., immune-related response criteria, RECIST1.1, modified RECIST).20,21 In response, in March 2017, the RECIST working group released a newly developed consensus guideline providing a standard approach to assessing solid tumor response to immunotherapy (iRECIST).20
One of the lessons learned with some targeted therapies includes the role reliable and relevant biomarkers can play in selecting patients who will substantially benefit from treatment with these therapies; comparable predictive biomarkers have yet to be clearly established for I-O agents.17 Some clinical trials have used tumor PD-L1 expression as an eligibility criteria; yet, data have shown the level of PD-L1 may be more prognostic than predictive in terms of response to treatment.2
More so, predicted response to I-O treatment based on PD-L1 expression has been found to vary across cancer types.22 Furthermore, to date there has been a lack of standardization for PD-L1 testing in terms of assays, cells tested, and cut-off thresholds.2,16
While significant focus has been placed on biomarkers, the influence of other factors such a tumor mutational burden and genetic abnormalities (e.g., mismatch repair deficiency [MMR]) on treatment response is garnering significant attention.16,22 As such, clinical development of I-O agents and patient outcomes could benefit from the following: 1) implementation of biomarker programs that allow for discovery of other predictive biomarkers, validation of current biomarkers, and development of companion diagnostics; and 2) incorporation of tests that evaluate mutational burden and genetic abnormalities.2,17,22
Previous studies have found that in academic and community settings, ineligibility is a barrier to accrual in 16% and 24% of screened patients, respectively. However, a recent analysis has suggested otherwise. In 2008, the National Cancer Institute Community Cancer Centers Program (NCCCP) developed a web-based log that collected data for patients (N=4,483) screened for select cancer trials between 2009 and 2012. Of those screened, 1,886 (42%) were ineligible due to issues with trial exclusion criteria; 1,771 (40%) patients were eligible but chose not to enroll; and 826 (18%) went on to enroll in one of the trials.
Reasons for non-enrollment were varied and crossed multiple domains (Table 5). Results of this analysis suggest that stricter eligibility criteria for many of the newer drugs under development, such as biomarker status and additional pathology samples, may be driving these changes. 23 In addition, with ongoing recent market approvals, the chance that patients are I-O naïve becomes slimmer; thus, trial protocol development should consider including patients previously treated with I-O therapy, perhaps as a separate cohort.2
Table 5. Top Reasons Patients Do Not Enroll in Select Cancer Trials23 Screened patients (N=4,486) Reasons (more than one could be selected) Patients ineligible n=1,886 (42%) Comorbidities (27%) Prior therapy (21%)Inadequate pathology sample (11%) Biomarker criteria (10%) Patients eligible, but did not enroll n=1,771 (40%) Patient declined participation n=944 (53%) No desire to participate (43%) Preferred standard therapy (40%) Perceived adverse effects (9%) Social issues (4%) Financial (3%) Insurance (3%) Provider declined to offer the trial n=570 (32%) Preferred standard of care (53%) Comorbidities/frailty (29%) Offered other trial (5%) Unaware of trial (5%) Lack of social support (5%) Other n=257 (15%) Urgent treatment needed (14%) Study suspended (1%)
In the era of molecularly-driven trials, it has been suggested that modernizing eligibility criteria may improve patient accrual and the generalizability of study results, and also streamline the drug clinical trial and approval processes.24 While no clear path to this modernizing strategy has been identified, an initiative spearheaded by the American Society of Clinical Oncology (ASCO) Cancer Research Committee has developed a set of recommendations designed to spur thoughtful conversations amongst stakeholders involved in developing clinical trial protocols about inclusion/exclusion criteria.24
Despite awareness that more patients could benefit from participating in cancer clinical trials, effective recruitment and accrual continue to be challenges. In fact, overall an estimated 18% of publicly funded cancer studies close due to failure to enroll an adequate number of patients or accrue less than 50% of target, three or more years after trial initiation.25 Lower accrual rates occur with cancer studies evaluating multimodality treatments, surgery, or radiation therapy; those evaluating new investigational agents or targeted therapies tend to have higher accrual rates.25
Low participation rates may contribute to the delayed rates of drug development, may impair the generalizability of trial results, and result in missed opportunities for patients to experience the potential clinical benefit of investigational agents.6,26 Numerous barriers to clinical trial participation have been identified including access to cancer trials (e.g., clinic availability, transportation, insurance, travel costs, child care), trial suitability and eligibility for participation, and physician and patient attitudes toward and knowledge of clinical trials.6 Several aspects of access as a barrier to participation are highlighted below.
Successfully enrolling oncology trial participants can be challenging since across the country many key cancer clinical trials are first conducted at large, urban cancer centers. For example, there are currently 69 National Cancer Institute (NCI)-designated Cancer Centers, which are located in 35 states and the District of Columbia – 62 of these provide patient care and 27 are also designated as National Comprehensive Cancer Network (NCCN) member institutions.27,28 As shown below (Figure 1), access to trials at these centers can prove trying for patients in rural and non-major metropolitan areas for a variety of reasons including travel-related hardships such as transportation, lodging, absences from work, and family care costs.
Figure 1. National Cancer Institute (NCI)-designated Cancer Centers

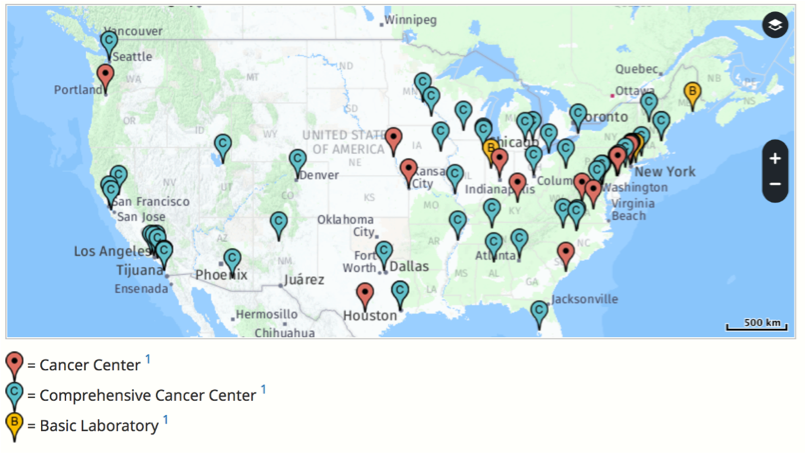
Source: https://www.cancer.gov/research/nci-role/cancer-centers/find
To help alleviate this burden and improve access, many sponsors of clinical trials now partner with site management organizations (SMOs) specializing in cancer clinical research that have developed networks of community cancer centers with experienced clinical investigators to recruit and provide care to patients in non-metropolitan settings.29
Additionally, many cancer centers have developed their own networks of cancer clinical trial sites to improve patient access and participation. For instance, the Fred Hutchinson/University of Washington Cancer Consortium is a research collaboration comprised of the Fred Hutchinson Cancer Research Center, the University of Washington, the Seattle Cancer Care Alliance, and Seattle Children’s Hospital. Recognized as an NCI-designated Comprehensive Cancer Center, this consortium facilitates access to cancer clinical trial participation through more than a dozen community and network sites throughout Washington, Oregon, Alaska, and Montana.30
Insurance coverage for participation in cancer clinical trials varies by plan type and state. For example, under the Affordable Care Act (ACA), private insurers are required to cover routine patient costs associated with eligible patient participation in approved, federally funded clinical trials. Similarly, patients enrolled in Medicare, TRICARE, and Veterans Affairs insurance receive coverage for qualified clinical trials.
However, those enrolled in Medicare Advantage or private Medicare managed plans face hurdles to participation compared with those receiving fee-for-service coverage.31 Medicaid is another major source of insurance coverage although, it is not mandated that Medicaid provide coverage of the routine costs associated with participation in clinical trials.1,31
Routine care costs are those that would be incurred regardless of clinical trial participation status. In contrast, research costs are specific to the clinical trial and include the cost of the intervention, additional doctor visits, and extra lab and imaging tests. Insurance generally does not cover research costs; however, study sponsors may. Personal expenses, such as transportation, lodging, and child care frequently are not covered.32,33
As such, it is important to recognize financial burden as a potential barrier for patient participation in I-O clinical trials. Data collected (2013-2014) for patients participating in clinical trials at the Massachusetts General Hospital Cancer Center found that patients incurred the following additional average monthly travel and lodging expenses: Massachusetts residents spent ≥$200 per month; New England regional patients spent ≥$300 per month; and out-of-region patients spent ≥$900 per month.33
Concerns about clinical trial costs for patients with cancer are real and may impact decisions to participate. A survey of more than 1,200 patients with cancer found nearly 40% of patients agreed with the statement “I’m afraid my insurance won’t pay for a clinical trial” and 30% agreed “I’m worried that I wouldn’t be able to afford the costs of treatment on a clinical trial.”34
Many cancer centers employ staff to facilitate connecting patients/families to internal/external resources for support (e.g., financial, transportation, housing). As an example, SCCA provides a housing guide for their patients that addresses transportation, housing, and housing expense needs. In addition, the National Cancer Institute (NCI) provides a web- and phone-based service to help link patients and their families to organizations that provide emotional, practical, and financial support services.
The clinical successes seen with I-O therapies demand that the clinical development process be optimized to reflect the unique responses observed with these new drugs. This process is challenging stakeholders to rethink development strategies across multiple domains such as utilizing novel clinical trial designs; redefining clinically meaningful endpoints and approaches to assessment; deploying new analytical approaches; modernizing patient eligibility requirements; and identifying additional factors to help guide patient selection to maximize treatment response (e.g., biomarkers, tumor mutational burden, genetic abnormalities).
Unfortunately, most patients diagnosed with cancer will never participate in a cancer clinical trial, representing a missed opportunity to receive treatment with a potentially more effective therapy. Increasing patient accrual/enrollment through improving patient, family, and healthcare provider education, outreach, access, and support goes a long way to ensuring the ultimate goal speeding the delivery of safe and effective I-O therapies to patients with cancer.

















