Author(s):


Across the country, cancer programs are working to improve how and when palliative care is introduced for patients with advanced disease. Recent studies continue to reinforce what has long been known: Early palliative care involvement enhances symptom control, improves patient and caregiver experience, and reduces avoidable emergency department visits and hospitalizations.1,2 When offered in the outpatient setting, palliative care strengthens communication and decision-making, helping patients receive care that aligns with their goals and values.3
Research also highlights that early palliative integration can reduce the total cost of care by avoiding unnecessary hospitalizations and intensive treatments near the end of life. These improvements in quality and affordability represent an important opportunity for oncology programs seeking to balance patient-centered care with sustainable resource use. Despite these benefits, palliative care remains underused. Many reports point to familiar barriers, such as limited staffing, fragmented workflows, prognostic uncertainty, and provider discomfort, which continue to delay referrals and can lead to missed opportunities for earlier support.4,5 These barriers often result in delayed palliative engagement, avoidable hospitalizations, and diminished quality at the end of life.
At WellSpan Cancer Institute, in York, Pennsylvania, these national trends were reflected in our program's data. Although clinicians understood the value of palliative care, the system's processes did not always prompt timely discussions. Early efforts relied on routine advanced-care planning conversations for every patient, regardless of disease stage. While this standardized practice encouraged awareness, it lacked clinical nuance and led to inconsistent outcomes.
Routine Conversations to Predictive Precision
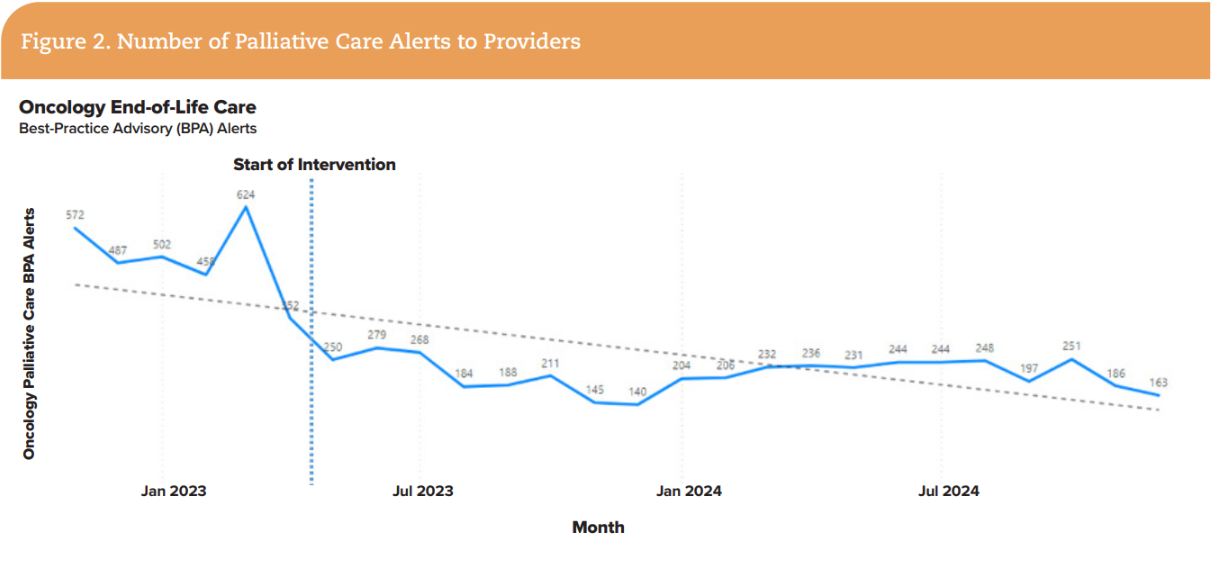
To improve timing and effectiveness, our oncology team transitioned from universal advanced-care planning conversations to an electronic health record (EHR) alert. The new alert was rule-based: If a patient had a stage IV cancer diagnosis and had not yet been referred to palliative care, the EHR would prompt the oncologist to consider a referral. While well-intended, this design proved too blunt; the alert fired frequently, creating alert fatigue and frustration. Provider feedback at Quality Management Council meetings described the system as "too much" and lacking meaningful discrimination. This feedback underscored the need for a more precise, context-aware alerting system that could distinguish between patients in stable condition and those at greater risk.
In response, the leadership team sought to balance outcomes with provider input. Within Epic, the health system's EHR, a predictive tool already existed but was not being actively used: the End-of-Life (EOL) Care Index, a validated model that estimates a patient's 12-month mortality risk using structured clinical and utilization data.
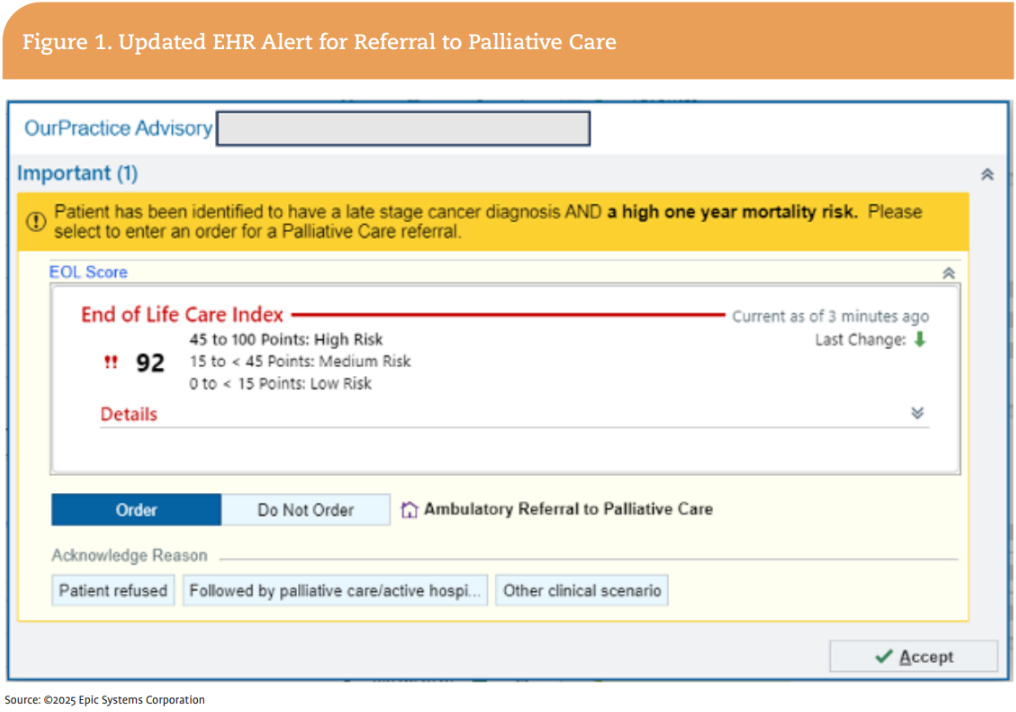
The innovation was not the model itself; it was the decision to leverage the model to refine the alerting logic as a test of change. The updated alert (Figure 1) would now trigger only when 3 requirements were met:
This integration transformed a generic reminder into a precision-guided prompt. Providers began receiving fewer alerts overall, but those they did receive were more relevant and clinically meaningful. One oncologist reflected, "Before, it felt like the system was interrupting me. Now it feels like it's helping me notice something important."

Aligning Quality, Cost, and Compassion
WellSpan's project was built around 3 aims:
These goals aligned directly with WellSpan's systemwide quality and value-based care priorities. Rather than viewing palliative care as a downstream service, the team reframed it as a proactive component of comprehensive oncology care, one that improves both patient experience and cost sustainability. This alignment not only advanced the organization's quality metrics but also reinforced its commitment to value-based oncology care, where improving outcomes and lowering cost are viewed as complementary goals rather than competing ones.
Building Trust Through Continuous Feedback
Implementation success depended on transparency and engagement. Data on alert frequency, referral rates, and early outcomes were reviewed regularly at Quality Management Council meetings. These discussions gave oncologists an opportunity to validate the alert's accuracy, interpret real-world patient examples, and refine how the system was used.
A palliative care physician reflected on the change, "We still meet some patients near the end of life, but now oncologists are introducing us much earlier. It gives us the chance to build a relationship, understand what matters most to patients, and support them through the course of their illness, not just at the very end."
Regular data review reinforced collaboration between clinicians and leadership. Over time, the focus shifted from tracking referral rates as a process metric to recognizing a decrease in inpatient utilization at the end of life, achieved through meaningful co-management with palliative care. This feedback loop built trust in the system and helped transform a data initiative into a shared clinical tool that supports both providers and patients.
Results and Impact
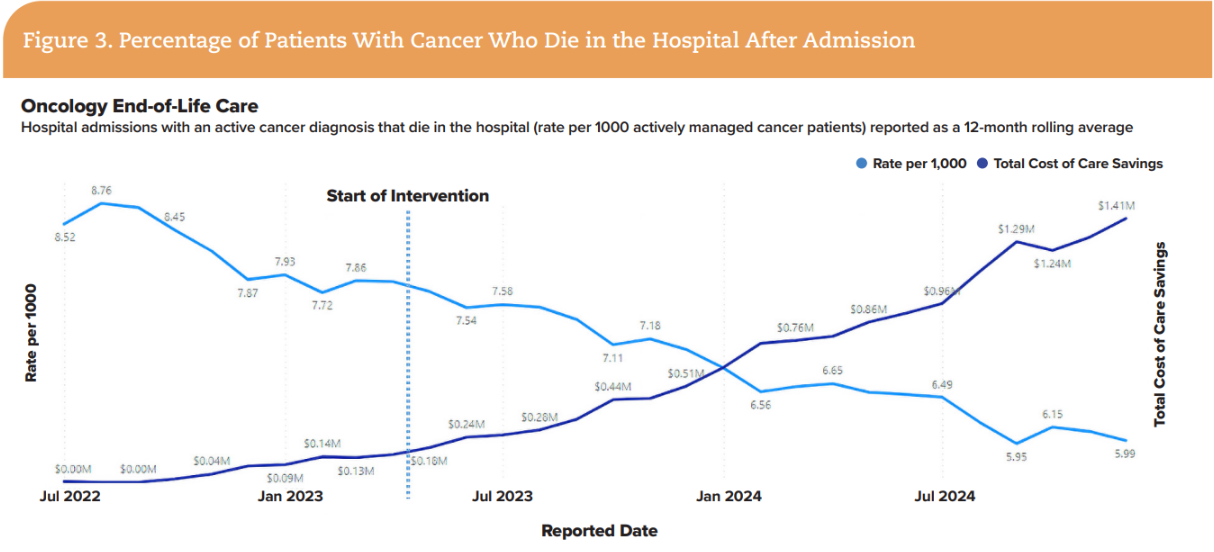
Since the machine-learning-informed clinical decision support alert went live in April 2023, measurable improvements have been observed:

A correlation analysis demonstrated a strong relationship between increased referrals and reduced in-hospital deaths (R²=0.953, P<0.001). This strong correlation suggested that the alert functioned not only as a technical enhancement but also as a behavioral cue, supporting timely, patient-centered action at the point of care. Together, these improvements demonstrated that predictive analytics could enhance—not disrupt—clinician workflow when thoughtfully designed around provider needs.
While the data show clear efficiency gains, their true meaning lies in improved patient experience. By identifying the right moment to introduce palliative care co-management, oncologists were able to ensure that patients received care aligned with their values and needs.
Simplicity in Design
From the outset, the team prioritized ease of use. The clinical decision support alert required each provider to acknowledge the prompt and complete 1 of 2 actions: initiate a palliative care referral or document a clinical reason the referral was not appropriate.
Equally important, the tool preserved physician autonomy. The alert did not prescribe a specific action; it simply brought forward information at the moment it was most relevant. This design supported reflection, without replacing provider judgment. This balance between data and empathy proved essential for sustained adoption. The clinical decision support prompt became not a compliance measure but a cue for awareness, a data-informed reminder to ensure that important conversations and co-management with a palliative care provider happened earlier in the patient's journey.
Advancing Health Equity and Affordability
Beyond workflow improvements, the initiative carried important health equity implications. The American Cancer Society Cancer Action Network's 2024 Survivor Views survey found that nearly half of insured cancer patients carry medical debt, often exceeding $5,000, and that Black patients are more likely to face debt collection. These findings underscore how resource-intensive care at the end of life can amplify financial hardship and perpetuate inequities in access to supportive services.
By encouraging earlier community-based palliative engagement, the clinical decision support tool supported both affordability and fairness. Because it draws on objective clinical data rather than subjective perception, the system promotes consistent referral patterns across all patient populations. The approach helps ensure that decisions about supportive care are based on medical need—not circumstance—reinforcing WellSpan's commitment to equitable, patient-centered care.
Lessons Learned
Several practical lessons emerged that may guide other cancer programs looking to implement similar predictive tools:
The project also underscored that innovation in oncology quality is as much about culture as technology. Progress depends on cultivating shared ownership of patient-centered goals and maintaining alignment between providers, data teams, and leadership. Ultimately, the initiative succeeded not because of technology alone but because it strengthened relationships between oncologists and palliative care teams, between data and decision-making, and between systems and patients.

Sustaining and Expanding the Model
Encouraged by these results, WellSpan Health System is expanding the approach beyond oncology to include other high-risk chronic disease populations, such as chronic obstructive pulmonary disease, congestive heart failure, and end-stage renal disease. These patient populations often face similar challenges in recognizing health decline early and avoiding non–goal-concordant care at the end of life.
By adapting the predictive framework and clinical decision support logic to these groups, WellSpan aims to create a systemwide approach to serious illness management, one that applies data intelligently to identify needs, prompt communication, and coordinate care across specialties.
This next phase represents a natural evolution of the work, from a focused oncology innovation to an integrated population-health strategy that uses predictive analytics to connect precision with compassion across the continuum of care.
Concluding Thoughts
The implementation of machine-learning-enabled clinical decision support at WellSpan Cancer Institute represents a promising intersection of analytics, empathy, and equity. By pairing a validated mortality prediction model with a thoughtful workflow design, the program achieved measurable gains in outcomes, reduced clinician alert burden, and improved cost efficiency while preserving the human connection that defines quality oncology care.
As health systems across the country confront rising cancer costs and workforce constraints, initiatives like this demonstrate that technology, when applied purposefully, can strengthen, not replace, the art of medicine. By guiding early conversations, fostering shared decision-making, and promoting equitable access to supportive care, predictive analytics can help redefine what good care looks like at the end of life.
Andrew Munchel, MSN, RN, OCN, CPHQ, is Oncology Quality Program Administrator at WellSpan Cancer Institute, WellSpan Health, York, Pennsylvania.
References



: A Proven Framework for Streamlined Cancer Care Delivery")





























