Author(s):
The integration of biomarker testing into routine cancer care has transformed therapeutic decision-making, particularly in gynecologic malignancies, where biomarkers such as BRCA1/2, MMR/MSI, HER2, HRD, and PD-L1 have become essential for guiding treatment selection. Across oncology, the scope and complexity of biomarker testing have expanded rapidly, with new prognostic and predictive markers emerging each year—a trend expected to continue for decades to come.1 However, national data reveal that testing rates and efficiencies often lag behind best-practice recommendations, resulting in missed opportunities to personalize therapy.2
Operational and logistical challenges compound these gaps. Variability in laboratory workflows, limited resources, and insufficient coordination among clinicians, pathologists, laboratory personnel, and the larger multidisciplinary team contribute to testing delays or failures. As the number of actionable biomarkers continues to grow, the need to strengthen the operational systems that support testing has become increasingly urgent.2
Despite strong evidence and established national guidelines,3 many oncology programs still face structural and systemic barriers that prevent consistent, timely, and equitable implementation of biomarker testing. Gaps in multidisciplinary coordination, electronic health record (EHR) integration, and reimbursement processes frequently lead to variability in practice across (and even within) institutions.
The Association of Cancer Care Centers (ACCC) launched a nationwide quality improvement (QI) initiative to evaluate and strengthen biomarker testing workflows in gynecologic oncology. Through structured workshops and facilitated implementation planning, the initiative aimed to integrate precision medicine principles into everyday practice across various clinical settings. Three geographically diverse cancer centers participated, representing both academic and community environments. Workshops guided the assessment of feasibility, identification of common barriers, and helped to generate actionable strategies for improvement of biomarker use over the course of 6 months.
Operationalizing Biomarker Testing in Gynecologic Malignancies


The educational initiative was designed to address a fundamental question: How can oncology programs translate the promise of precision medicine into consistent, guideline-concordant care for all patients with gynecologic malignancies? While biomarker testing has become integral to therapeutic planning, the process of ordering, interpreting, documenting, and acting on results is often fragmented across departments, specialties, and even care settings. Coordinating processes with external vendors and integrating documented, actionable results into the internal EHR is another frequently encountered obstacle.
The overarching objective of the ACCC-led program was to support multidisciplinary teams in identifying practice gaps, developing site-specific improvement plans, and advancing equitable access to precision medicine. Supported by a multidisciplinary steering committee with expertise in gynecologic oncology, pathology, genetics, pharmacy, and QI, each site participated in a 3-phase process.
This structured yet adaptable model provided a foundation for sustainable process improvement, encouraging each site to align testing workflows with current evidence-based guidelines while adapting solutions to their institutional realities
On-Site QI Workshop Design
The QI workshops were structured as immersive, data-driven sessions rather than didactic training. By anchoring discussions in each site’s own baseline data, participants were able to visualize where breakdowns occurred, from test ordering and result reporting to communication of findings and financial/reimbursement concerns. Facilitated by ACCC QI professionals, each site’s multidisciplinary team met in person for a full-day session focused on the following objectives:
Review baseline data on biomarker testing rates, EHR workflows, and patient access barriers
Identify and prioritize key challenges, such as inconsistencies in ordering responsibility, lack of reflex testing protocols, or reimbursement delays
Develop a site-specific aim statement describing the measurable improvement goal, timeline, and scope
Map current-state workflows to visualize testing processes and identify opportunities for automation or streamlining
Outline an implementation plan guided by the PDSA framework to test and refine small-scale interventions over time.
This approach fostered collaboration across departments that rarely had dedicated time for collective process review. Importantly, the workshops also emphasized the role of financial navigation and equity, recognizing that access to biomarker testing is influenced not only by clinical infrastructure but also by patients’ insurance coverage, out-of-pocket costs, and geographic barriers.
The QI workshops thus served as both an educational and operational platform, equipping participating programs with the tools to build sustainable, systems-level solutions.
Montana: Coordinating Care Across Rural Geographies and Health Systems
In Montana, where geographic distance often separates patients from subspecialty cancer care, Logan Health in Kalispell had partnered with colleagues at Billings Clinic to strengthen care coordination for patients with gynecologic malignancies. The collaboration brought together complementary expertise and infrastructure. Billings Clinic, home to a gynecologic oncology–focused tumor board, contributes deep subspecialty knowledge in surgical oncology and molecular diagnostics. Logan Health offers a strong multidisciplinary team (ie, genetics, nursing, navigation, pathology, and medical oncology) committed to expanding access to high-quality, timely care for patients across rural western Montana.
Historically, communication between the 2 programs had been limited, particularly around tumor board participation, treatment decision-making, and role clarity in ordering and follow-up for biomarker testing. The ACCC-led workshop provided a dedicated forum to assess current processes, identify shared strengths, and map out a collaborative path forward.
During the workshop, teams identified a clear overarching challenge. Although both programs had strong individual capabilities, they lacked an integrated, standardized process for biomarker testing across ovarian, endometrial, and cervical cancers. Contributing factors included fragmented referral pathways, variations in guideline interpretation by discipline, limited interoperability between EHRs, and uncertainty about who was responsible for ordering and following up on test results. These issues occasionally led to duplicated or delayed testing, increased logistical burden for patients and caregivers, and, at times, missed opportunities for guideline-concordant therapy selection.
Building from this problem statement, Logan Health and Billings Clinic defined a shared QI goal: develop a unified biomarker testing process with clearly defined roles and communication pathways. Their collaborative plan emphasized both achievable “quick wins” and longer-term infrastructure development. Early action steps included creating a current-state process map, developing a standard referral pathway for all gynecologic cancers, ensuring that somatic testing results were shared with the genomics nurse practitioner and integrated into the EHR, and identifying disease-specific patient education resources on biomarker testing. The team also began integrating Logan Health’s nurse navigator into regular cross site meetings and established a recurring schedule for its multidisciplinary team to participate in Billings Clinic’s gynecologic oncology tumor board.
Longer-term goals included standardizing which laboratories are used for testing, embedding disease-specific patient education materials into the EHR, and exploring in-house immunohistochemistry (IHC) capabilities for select biomarkers such as PD-L1. The sites also discussed financial navigation as a key area for future attention, noting opportunities to partner with Billings Clinic financial advocates to support patients at Logan Health facing coverage or prior authorization challenges.
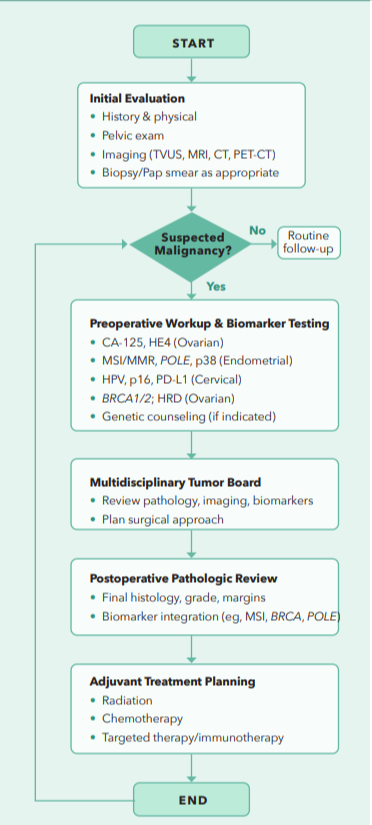
By month 3, the Logan–Billings partnership had achieved a major milestone: the creation of a diagrammed biomarker testing workflow with assigned responsibilities across both organizations (Figure 1). This shared roadmap now serves as the foundation for continued process refinement. It has strengthened communication and collaboration between 2 key cancer care providers that serve patients across Montana’s vast geography.
FIGURE 1. Diagrammed Biomarker Testing Workflow Developed by Logan Health and Billings Clinic

Ohio: Standardizing Established Biomarker Testing Practices Across Providers in a Large Health System
At TriHealth Cancer & Blood Institute in Ohio, a large integrated health system serving diverse urban and suburban populations, the QI workshop centered on refining already well-established biomarker testing processes to maintain alignment with evolving standards of care in gynecologic oncology. The health system entered the initiative with multiple strengths, including the use of an EHR system with built-in genomics integration and robust data analytics capabilities, supported by a highly responsive information systems team. The institution also benefits from 8 dedicated cancer genetic counselors (GCs) with urgent referral workflows, frequent gynecologic and molecular tumor boards that review all new and recurrent cases, and a clear process for annual and as-needed workflow updates.
TriHealth’s commitment to equity and care access is evident in its use of the Social Vulnerability Index to identify at-risk populations, implementation of mobile phlebotomy, and telehealth genetic counseling visits (including urgent next-day appointments) to reach patients across its network. Financial navigation and fertility counseling were routinely incorporated into the patient’s journey. Together, these systems created a strong foundation for patient-centered care.
During the workshop, participants acknowledged that while strong workflows existed, the rapid pace of advances in biomarker science necessitated frequent, structured updates to preserve standardization and reduce provider-level variability. The group’s discussions focused on ensuring that ovarian, endometrial, and cervical cancer workflows remained comprehensive, consistent, and aligned with current guidelines.
TriHealth’s QI problem statement reflected a balance between established infrastructure and ongoing evolution. While strong workflows and regular updates were in place, the rapidly changing biomarker landscape required continual revisions to ensure alignment with best practices and to minimize variation in provider adherence. Without this, there remained a risk that some patients might not receive uniform access to testing or clinical trial opportunities.
For ovarian cancer, TriHealth aimed to integrate FOLR1 testing into the default Tempus XT order, eliminating the need for a separate pathology order. TriHealth acknowledged its current high compliance with germline and somatic testing, and voiced enthusiasm for continuing that success. For endometrial cancer, the team seeks to continue using breast scoring for HER2 IHC to determine trial eligibility while planning to adopt gastric scoring for therapeutic decisionmaking. Participants also plan to ensure next-generation sequencing (NGS) testing is carried out for all stage III or recurrent cases and are aiming to include POLE testing in routine workflows. Although documentation of genetic counseling in the EHR was generally strong, participants noted variability in endometrial cases. To address this, TriHealth plans to create smart phrases, and a survivorship care plan prompts them to capture whether genetic counseling was offered, accepted, or declined—providing a more consistent record across disease sites and providers.
“We created a new workflow for each of these cancers [for] germline and somatic [testing] ... We’ll start looking at compliance as of January 1, 2026 and we’ll assess it twice yearly.” – Precision Medicine Director, TriHealth Blood & Cancer Institute
For cervical and other gynecologic cancers, the team endorsed universal reflex PD-L1 testing and expansion of reflex testing protocols to include these tumor sites. Additional goals included incorporating HER2 testing (using gastric scoring) and NGS for recurrent or stage IVb cases. The team also identified financial considerations and patient education as priorities, particularly in the context of addressing fears related to germline testing and insurance coverage. GCs plan to distribute educational handouts that explain protections under the Genetic Information Nondiscrimination Act (GINA), billing FAQs, and referral information.
By month 6, TriHealth reported steady progress toward implementation of its updated biomarker testing workflows using a structured, multi-cycle QI approach. An initial planning and baseline assessment phase focused on reviewing data charts, conducting pre-assessment activities, and prioritizing improvement actions. The second cycle, spanning October through December 2025, marked the systemwide “go-live” of revised workflows across gynecologic oncology and pathology teams, with defined metrics established to assess pre- and post-intervention performance and early process adoption.
Key implementation activities included the rollout of standardized biomarker testing workflows, deployment of EHR smart phrases to document genetic counseling discussions, and distribution of patient education materials. Progress was supported by strong multidisciplinary buy-in, dedicated staff time, embedded GC participation in tumor boards, and centralized oversight by a precision medicine lead. Alignment with Commission on Cancer (CoC) Standard 7.3 further reinforced accountability and enabled integration of biomarker testing metrics into accreditation reporting.
As TriHealth enters an early monitoring phase in January 2026, the team anticipates iterative refinement of workflows and targeted reeducation as needed, recognizing that continuous adaptation is essential to maintain guideline-concordant care in a rapidly evolving biomarker landscape. The QI workshop underscored that even mature systems benefit from structured opportunities to reassess, refine, and standardize processes in response to new clinical evidence.
South Carolina: Strengthening Financial Transparency and Molecular Testing Coordination in a Community-Based Cancer Program
At Spartanburg Regional Healthcare System in South Carolina, the biomarker testing QI effort focused on refining wellestablished operational processes within a busy community oncology network while addressing persistent financial and coordination barriers. The program already possesses a strong infrastructure: biomarker testing is fully integrated into the EHR, workflows for ordering and processing are clearly defined, and multidisciplinary collaboration among oncologists, pathologists, navigators, and GCs ensures that testing results are rapidly incorporated into treatment planning. Clinical guidelines, such as those from the National Comprehensive Cancer Network® (NCCN®), are consistently used to identify eligible patients, and dedicated molecular tumor boards support alignment in decision-making across teams.
Despite these strengths, the team identified several structural challenges. Among the most significant is the Medicare 14-day rule, which requires that molecular and genetic tests ordered within 14 days of a hospital encounter be billed through the hospital rather than the reference laboratory performing the test. Although initially designed to clarify billing ownership and prevent duplicate claims, this policy often delays test ordering and results in limited availability. External laboratories must hold specimens until the 14-day window has passed before submitting claims for reimbursement, creating logistical bottlenecks that slow turnaround times and complicate coordination among clinical, pathology, and billing teams. These issues are particularly acute for newly diagnosed patients with Medicare, where timely test results are critical for initiating first-line therapy. In general, the Spartanburg team described administrative and billing workflows as opaque, citing frequently limited insight into reimbursement status or payment denials.
The team highlighted additional challenges related to staffing shortages on the histology team. Although gradually improving, the lack of sufficient personnel occasionally slowed specimen processing for multiple send-outs. Because most biomarker assays were performed at external laboratories, the program incurred additional costs, experienced longer turnaround times, and occasionally encountered discrepancies in biomarker reporting among vendors. Finally, the team noted that molecular tumor board meetings had become less consistent, reducing opportunities for comprehensive review of complex molecular results.
The QI workshop prompted the development of a multifaceted improvement plan to address both operational efficiency and financial sustainability. Key priorities include reestablishing a regular molecular tumor board and consistently securing external consultation for complex cases. Other priorities focused on strengthening billing transparency by engaging compliance and finance leaders as well as exploring vendor diversification to ensure competitive pricing and comprehensive NGS testing coverage. The team also identified opportunities to bring specific assays (eg, IHC, HER2 fluorescence in situ hybridization [FISH], and possibly POLE testing) in-house to reduce both cost and turnaround time.
By month 6, the Spartanburg team reported meaningful progress toward its QI goals. The precision medicine team established standing biweekly meetings to review progress, address barriers, and set near-term priorities. The organization engaged external consultants to conduct a comprehensive audit of its molecular billing workflows, resulting in ongoing corrections of CPT codes, revenue routing, and charge master reconciliation. These updates are being implemented through daily ticketed changes in collaboration with information technology and laboratory billing teams, which were identified as essential partners in ensuring accurate and timely reimbursement.
“We added an operational FTE this year that [will organize a molecular tumor board] as part of their job role ... We also noted that we were not properly charging on some of our cases.” – Precision Medicine Director, Spartanburg Regional Healthcare System
Looking ahead, Spartanburg anticipates completing the billing optimization phase in early 2026, after which efforts will shift toward the formal establishment of a molecular tumor board. The team identified interest in benchmarking with peer institutions that participate in multicenter molecular tumor boards as a priority area for future collaboration. Longer-term initiatives will focus on designing a QI intervention around financial navigation and reimbursement workflows, leveraging tools such as ACCC’s Financial Advocacy Network to benchmark best practices. The team plans to incorporate updated NCCN and College of American Pathologists guidelines (particularly the revised HER2 criteria for endometrial cancers) into reflex testing protocols and to continue stabilizing the histology and pathology navigation workforce. Collectively, these changes aim to enhance transparency, reduce delays, and ensure that financial considerations do not limit timely guideline-concordant biomarker testing.
Spartanburg’s experience highlights the distinct challenges faced by community oncology programs operating within complex reimbursement environments. Their initiative demonstrates that high-quality precision medicine requires not only strong clinical workflows but also robust administrative and financial systems that support equitable access to care.
Implementation of these process improvements will continue through early 2026, with metrics focused on turnaround times, reimbursement recovery, and reestablishment of molecular tumor boards. Lessons emerging from Spartanburg’s work are informing broader discussions on how community-based cancer programs can strengthen financial infrastructure while sustaining the pace of biomarker innovation.
Conclusion
Embedding precision medicine into gynecologic oncology requires more than just access to biomarker testing; it demands operational systems that ensure every eligible patient receives timely, guideline-concordant care. Across 3 geographically and structurally diverse cancer programs, this nationwide QI initiative demonstrates that data-driven, multidisciplinary collaboration can uncover barriers that might otherwise remain invisible within routine workflows.
Each site’s experience illuminated unique challenges: for Logan Health and Billings Clinic, geographic distance and inter-health system coordination; for TriHealth, the need to maintain consistency amid rapidly evolving biomarker standards; and for Spartanburg, financial and operational complexity driven by reimbursement policies such as the Medicare 14-day rule. Yet, Despite these differences, all teams share a common goal—to make precision medicine a reliable, reproducible part of everyday gynecologic cancer care.
Early successes include the creation of standardized testing workflows, renewed communication across disciplines, strengthened financial navigation, and improved clarity regarding ordering responsibilities. Perhaps most importantly, the initiative fostered a culture of shared accountability, empowering each team to view biomarker testing not as a discrete task, but as an integrated element of comprehensive, patient-centered oncology care.
Implementation and monitoring will continue through early 2026, with participating centers evaluating the impact of their interventions on testing rates, turnaround times, reimbursement recovery, and treatment decisionmaking. As these efforts mature, lessons learned will inform future initiatives designed to expand equitable care across additional tumor types and practice settings. By aligning infrastructure, education, and logistical planning, cancer programs can transform precision medicine from a specialized endeavor into a sustainable standard of care.
References



: A Proven Framework for Streamlined Cancer Care Delivery")





























