Presented at the 2021 ASCO Quality Care Symposium, September 24 - 25, 2021.
Authors
Matthew Smeltzer, Percy Lee, Joseph Kim, David R. Spigel, Brendon Matthew Stiles, Alexander I. Spira, Ravi Salgia, Howard West, Michelle Shiller, Elana Plotkin, Lorna Lucas, Leigh Boehmer
University of Memphis, School of Public Health, Memphis, TN; University of Texas MD Anderson Cancer Center, Houston, TX; MCM, Newton, PA; Sarah Cannon Research Institute/Tennessee Oncology, Nashville, TN; New York Presbyterian Hosp, New York, NY; US Oncology Research/Virginia Cancer Specialists, Fairfax, VA; The University of Chicago, Chicago, IL; Swedish Cancer Institute, Seattle, WA; Pathologists Bio-Medical Laboratories, Dallas, TX; Association of Cancer Care Centers, Rockville, MD
Background
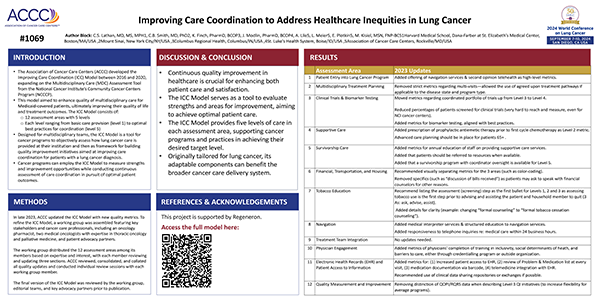
Quality improvement (QI) in cancer care delivery requires understanding the setting, clearly defining problem(s), and identifying targeted solutions. The Association of Cancer Care Centers (ACCC) conducted a national project to identify and provide guidance on key issues in care for patients with stage III/IV non-small cell lung cancer (NSCLC). We report the problems and solutions identified after a mixed-methods baseline data evaluation.
Methods
The multi-phase ACCC QI initiative was guided by an expert steering committee. A request for applications was advertised to all ACCC programs, with committee members ranking each site in pre-specified categories (ex., replicability, practice champion engagement). After selection of sites, baseline data assessed programs’ patient populations, current care delivery practices, processes of care, and biomarker testing rates. A full-day workshop was conducted with multidisciplinary team members and expert faculty to review baseline data, refine problem statements, and identify site-specific QI solutions.
Results
The 6 participating US sites were regionally diverse with a rural/urban mix. In baseline data, median patient ages were 65-72 years and patients treated were 50% stage III/50% stage IV. Biomarker testing practices, use of multidisciplinary tumor board, and clinical care pathways varied across sites. Five key QI areas were identified: 1. Management of immune related adverse events (irAE), 2. Biomarker testing, 3. Emergency visit management (EVM), 4. Access to clinical trials, and 5. Smoking cessation. Two sites identified problems with irAE management during immunotherapy (IT). The first identified needs for proactive symptom identification, assessment, and management. Solutions included: 1. a patient questionnaire to identify early signs of irAEs and 2. pilot testing a nurse-administered questionnaire. A second site identified that front-line clinicians may not be properly identifying possible irAEs. Solutions included: 1. form an IT toxicity working group and 2. educate front-line clinicians about irAEs. Two sites focused on biomarker testing. The first problem identified was inefficient tracking of testing results. Solutions were: 1. assign a nurse navigator to track, enter, and communicate test results and 2. proactively coordinate appointments for patients with positive test results. The second site identified delayed care when inadequate tissue was obtained. Solutions included: 1. pathology-driven reflex testing and 2. liquid biopsy order at diagnosis. Similar problems/solutions were developed for EVM, clinical trial access, and smoking cessation.
Conclusions
Challenges in lung cancer care delivery can be identified and addressed using an intentional QI approach. Clearly defining the problem and identifying potential solution(s) are critical steps and should occur before implementation.
Acknowledgements
ACCC would like to thank our project partners: LUNGevity, International Association for the Study of Lung Cancer (IASLC), and American College of Chest Physicians (CHEST).
Funding
This project is supported by AstraZeneca.
 ACCCBuzz Blog
ACCCBuzz BlogBy Molly Kisiel, MSN, FNP-BC
April 16, 2024