Author(s):
Contralateral prophylactic mastectomy is as a surgical procedure in which the healthy breast is removed after a diagnosis of breast cancer in the other breast. Bilateral mastectomy is a surgical procedure in which both breasts are removed at the same time, typically to treat and/or prevent breast cancer. Over 8 years, from 2005 to 2012, the rate of bilateral mastectomy tripled, and demand for this surgery continues to increase.1 There are various reasons patients desire contralateral prophylactic mastectomy or bilateral mastectomy, including symmetry, risk reduction, and improved access to reconstruction. Rates of bilateral mastectomy for unilateral, early-stage disease have increased, with a concurrent ease of access in reconstructive procedures over the same time.2 Qualitative studies point to patient concern about recurrence, use of preoperative breast magnetic resonance imaging, and higher educational attainment as factors associated with the rate of contralateral prophylactic mastectomy.3 However, contralateral prophylactic mastectomy has been shown to increase operative complications4 and inherently increases operative times. With an increased frequency in bilateral mastectomy, there is a need to ensure these procedures are performed safely and efficiently to optimize outcomes for patients and hospital systems.
Despite the increasing frequency of bilateral mastectomy, there is a lack of data evaluating how contralateral prophylactic mastectomy affects productivity in a surgical setting. Dual surgeon approaches have been used in various other surgical subspecialties; research suggests that this technique may effectively reduce operative times and complications associated with complex bilateral procedures, leading to improved outcomes.5,6 DIEP flap reconstruction is a breast reconstruction surgery that uses a patient’s own abdominal skin, fat, and blood vessels to reconstruct the breast, while preserving the abdominal muscles. Dual surgeon DIEP flap reconstructions, for example, have been found to decrease operative time, average patient length of stay, and postoperative complications.7 There is a lack of research on dual surgeon bilateral mastectomy and its impact on surgeon productivity and operative time.
A previous study surveyed practicing breast surgeons to learn their opinions regarding the dual surgeon bilateral mastectomy technique and to assess the current nationwide practice patterns.8 Based on that survey, some reported benefits of the dual surgeon technique were time savings, cost savings, opportunity to learn techniques, and mentoring opportunities. With increased interest in the dual surgeon technique, additional studies have demonstrated reduced operative time for bilateral mastectomy with no difference in complication rates.9
Our study aims to evaluate dual surgeon bilateral mastectomy and modeled single surgeon bilateral mastectomy to compare overall operative time and the number of cases scheduled per day. We also compare complication rates between primary and secondary surgeon sides for dual surgeon bilateral mastectomy.
Methods
Our team at Luminis Health Anne Arundel Medical Center performed a single-center retrospective chart review of patients who underwent simple/total, skin-sparing, or nipple-sparing dual surgeon bilateral mastectomy from 2021 to 2023 for breast cancer or prophylaxis. Patients who underwent reconstruction (with implants or tissue expanders) or no reconstruction were included. Patients who under-went nerve grafting, flap reconstruction, or had stage IV disease were excluded. The electronic health record was used to collect patient variables, including age, BMI, race, ethnicity, smoking status, and comorbidities. Time from the initial newly diagnosed cancer visit to surgery was calculated. Mastectomy type, nodal surgery type, receipt of neoadjuvant chemotherapy, and receipt of immediate reconstruction were recorded. Surgical data including total operative time and 30-day complication rates were obtained. Postoperative notes were reviewed to determine hospital length of stay and capture possible subsequent surgical complications such as abscess, cellulitis, hematoma, skin necrosis, skin ischemia, seroma, pulmonary embolism, and deep vein thrombosis. Whether the complication was present on the primary surgeon side or secondary surgeon side was noted. Operative time was defined as the time from surgeon entry to surgeon exit from the operating room. Primary surgeon operative time included time for axillary surgery. Because our cancer center had few single surgeon bilateral mastectomy cases, the hypothetical/modeled single surgeon case time was calculated as the primary surgeon’s median operative time added to the secondary surgeon’s median operative time.
Descriptive statistics were performed to assess patient and surgical characteristics for the study population. The operative time for the primary and assisting surgeons was measured in minutes as average ± standard deviation and median (25th-75th percentile). Rates of complications on the primary and assisting surgeon sides were compared using Chi-square tests. Fisher exact test was performed when the Chi-square assumptions were unmet. Statistical analysis was performed in SPSS v28.0 (IBM Corp, Armonk, NY). Statistical significance was assessed at P less than .05.
Results
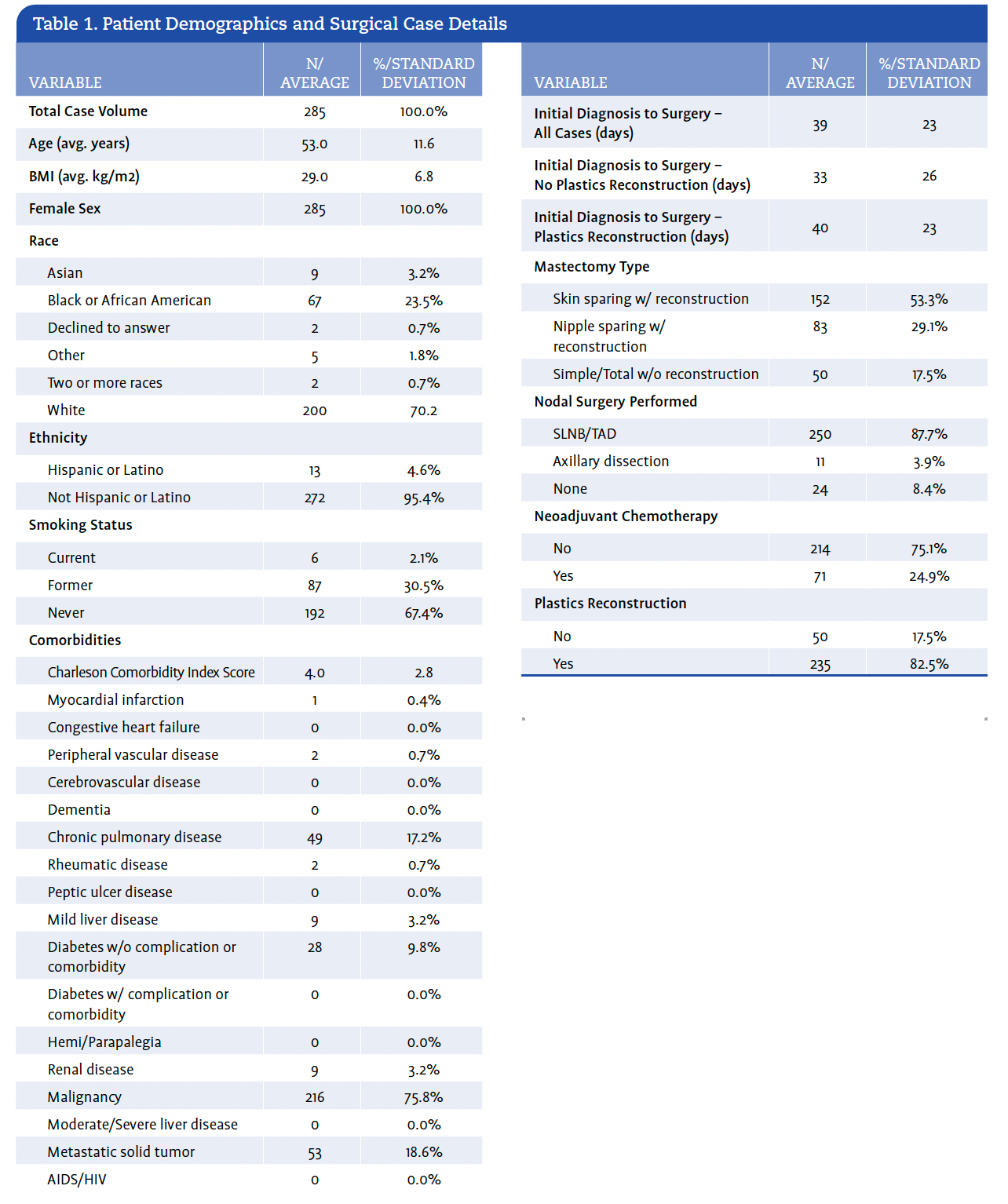
We identified 285 cases meeting the inclusion criteria. Immediate reconstruction was performed in 235 of the patients (82.5%). Neoadjuvant chemotherapy was given in 217 of the patients (24.9%). Of all patients, 152 (53.3%) had skin-sparing mastectomies with reconstruction, 83 patients (29.1%) had nipple-sparing mastectomies with reconstruction, and 50 patients (17.5%) had simple/total mastectomies without reconstruction. Sentinel lymph node biopsy or targeted axillary dissection was performed in 250 patients (87.7%), axillary lymph node dissection was performed in 11 patients (3.9%), and no axillary nodal surgery was performed in 24 (8.4%) of patients (Table 1). Targeted axillary dissection is a procedure that combines sentinel lymph node biopsy with targeted removal of a previously biopsied positive lymph node.10 In all cases of unilateral cancer, the primary surgeon operated on the side with cancer.
The median operative time for the primary surgeon was greater than the median operative time for the secondary surgeon (102 ± 33 vs 76 ± 31 minutes) (Table 2). Thus, the actual median operative time for dual surgeon bilateral mastectomy was 102 minutes (secondary surgeon simultaneous with primary surgeon). The modeled time for single surgeon bilateral mastectomy was 178 minutes (102 + 76).
The median operative time values were used to create a model of a typical operating room day with various surgeon scenarios (Figure 1). One breast surgeon and one plastic surgeon could perform 2 bilateral mastectomies with reconstruction in a day. When an additional breast surgeon is added, productivity increases, and the breast surgeons can complete 2 bilateral mastectomies with reconstruction and an additional dual surgeon bilateral mastectomy without reconstruction. When a second operating room is added, the 2 breast surgeons and 1 plastic surgeon can complete 4 bilateral mastectomies in a day (3 with reconstruction and 1 without reconstruction) and some more minor cases.
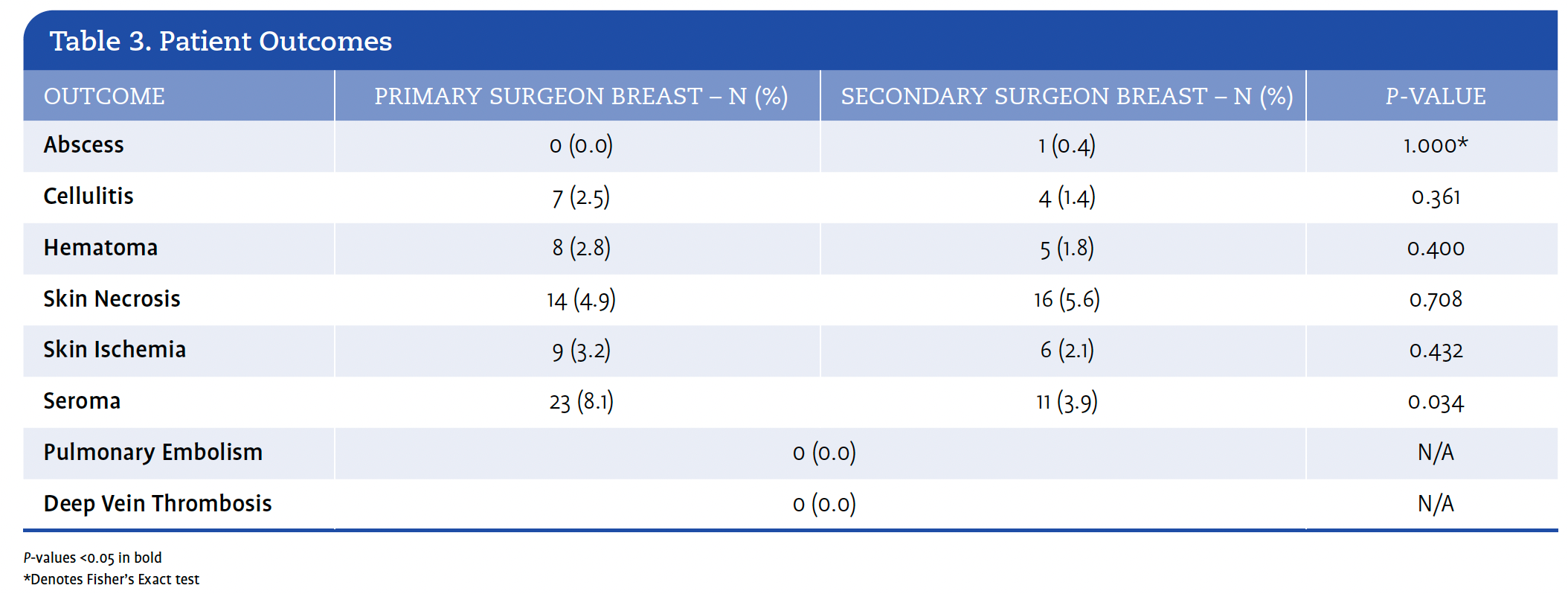
Overall time from initial diagnosis to surgery was 39 ± 23 days. There was no significant difference in time to surgery between patients who underwent plastics reconstruction (40 ± 23 days) and those who did not (33 ± 26 days; P = .106) (Table 1). Complication rates were comparable between the primary surgeon and secondary surgeon sides, apart from postoperative seroma, which was more common on the primary surgeon side (8.1% vs 3.9%; P = .034) (Table 3).
Discussion
This study is one of the most extensive evaluations of dual surgeon bilateral mastectomy to date. Our findings suggest that the dual surgeon approach to bilateral mastectomy can reduce operative time and increase productivity compared to the single surgeon approach. Improved efficiency in the use of OR time could contribute to shorter time from diagnosis to surgery, a metric that authors Wiener et al linked to overall survival in a study of the data from the National Cancer Database. The study reported that patients undergoing reconstruction had longer median times to surgery (38 days) than patients who did not undergo reconstruction (29 days).11 Increased case through-put via the use of 2 surgeons for bilateral mastectomies could lead to reduced time to surgery for patients with breast cancer.






Dual surgeon bilateral mastectomy is an efficient way to schedule the plastic surgeon, as the plastic surgeon has less wasted nonoperative time between cases when an additional breast surgeon is operating. Plastic surgeon availability can be rate-limiting at many programs; thus, improving plastic surgeon efficiency may contribute to shorter time from diagnosis to surgery.
Another benefit of dual surgeon bilateral mastectomy is that it reduces anesthesia time on average compared to single surgeon procedures. Longer anesthesia time has been linked to increased rates of postoperative nausea and vomiting, with 1 study showing that a 30-minute increase in duration predicted a 59% increase in the incidence of this adverse event.12 In our experience, postoperative nausea and vomiting is a primary reason for overnight observation in a case where same-day discharge had been planned. Thus, reduced operative time may improve patient experience and increase the likelihood of successful same-day discharge. In addition to the elevated risks of postoperative nausea and vomiting, longer surgical duration has also been linked to increased risk of venous thromboembolism.13
Dual surgeon bilateral mastectomy has the additional benefit of working with peers, which may afford opportunities for mentoring and learning new techniques. A survey of members of the American Society of Breast Surgeons found that this approach was more likely to be used in academic, breast-only practices and in groups of 5 or more breast surgeons. For those interested in the dual surgeon bilateral mastectomy technique, mentoring, being mentored, and learning new techniques were some of the reasons surgeons were interested in the approach.8 Although mentorship is vital for surgeons, the lack of mentorship is quite common in surgical practice for new surgeons. In a survey of new surgeons, approximately one-third reported they lacked mentoring opportunities when they started.14
A potential negative of the dual surgeon bilateral mastectomy approach is its impact on the second breast surgeon’s schedule. The second surgeon cannot see clinic patients or perform their own operation as the primary surgeon when participating in this procedure. In a 2-room scenario (Figure 1, Model 5), it is often efficient for the second surgeon to do a minor case in room B, while the dual surgeon bilateral mastectomy is started in room A. Second surgeon involvement is also easier if more than 1 dual surgeon bilateral mastectomy is scheduled in a day or if the clinic and operating room are relatively close to each other. With more surgeons involved in each surgery comes the potential for increased complexity in coordinating multiple surgeons and oper-ating room schedules. A potential downside of dual surgeon bilateral mastectomy is an increased time from diagnosis to operating room if the schedules of numerous surgeons must be coordinated.
Seroma was the only complication that differed in frequency between sides, occurring more often on the primary surgeon’s side (23 vs 11; P = .034). This was likely due to axillary surgery being performed more frequently on that side.
This study was limited by the fact that it was a single-institution retrospective review. The lack of single surgeon bilateral mastectomy cases also limited the study. Instead of comparing actual single surgeon to actual dual surgeon operative time, the single surgeon operative time had to be calculated based on the dual surgeon operative time. This study was also limited by the fact that operative time was defined as the time from surgeon entry to surgeon exit from the operating room, and it was not the true time that the surgeon was operating. In addition, information about patient satisfaction regarding symmetry and cosmesis following the dual surgeon approach was not collected. It was not possible to compare patient satisfaction and cosmesis between the dual surgeon and single surgeon approaches.
Dual surgeon bilateral mastectomy and the availability of 2 operating rooms have an amplifying effect because with 2 operating rooms, the abbreviated time for dual surgeon bilateral mastectomy (compared to single surgeon bilateral mastectomy) allows for more efficient use of both rooms. Figure 1 illustrates that when an additional breast surgeon is added to 1 operating room (Model 2), 2 additional mastectomies can be completed in a day (2 bilateral mastectomies with reconstruction and 1 bilateral mastectomy without reconstruction). When an additional operating room is added with 2 breast surgeons (Model 4), 5 bilateral mastectomies may be completed in a day (4 with reconstruction and one without reconstruction).
In summary, adoption of the dual surgeon bilateral mastectomy approach has many benefits, including reduced anesthesia time, more efficient use of operating rooms, more efficient use of breast and plastic surgeon time, mentorship opportunities for surgeons, and possible reduced time to surgery. Efficient operating room and plastic surgeon utilization is compounded by dual surgeon bilateral mastectomy when used in conjunction with 2 operating rooms. Based on these data, surgeons and patients can benefit from the implementation of dual surgeon bilateral mastectomy. Furthermore, these data can be used to advocate for 2 operating rooms at the institutional level, which, combined with the dual surgeon approach, may lead to more efficient use of operating rooms and surgeon time, and potentially more timely delivery of surgical care.
Eve Paxton, DO, is a breast surgical oncologist at Lakeland Regional Health in Lakeland, Florida. Carolina Baz, MD, is a general surgery resident; Rubie Jackson, MD, MPH, FACS, is a member of the breast surgical oncology faculty; Justin Turcotte, PhD, is a statistician and director of Surgical and Orthopedic Outcomes & Research; Steven Woodward, MD, is a member of the breast surgical oncology faculty; and Meghan Milburn, MD, FACS, is the chief of Breast Surgery at Medstar Franklin Square Medical Center in Baltimore, Maryland.
References