Author(s):
The International Classification of Diseases (ICD) is a system for classifying causes of morbidity (disease) and mortality. To reflect changes in medical nomenclature, improved understanding of the causes of disease, and identification of new diseases, new editions of the ICD are issued periodically by the World Health Organization (WHO), the copyright holder of ICD-10. The 10th edition of the ICD, Clinical Modification (CM) known as ICD-10-CM,1 went into effect in the US on October 1, 2015, the 11th edition is current in Europe, but the US has not advanced to that edition yet. Organizations that qualify as “covered entities” under the Health Insurance Portability and Accountability Act (HIPAA) are required to use ICD-10-CM codes on health insurance claims for services rendered on or after that date.
ICD-10-CM is a diagnosis coding system used by all providers, including both clinicians and hospitals. ICD-10-PCS (Procedure Coding System) is used by hospitals for reporting inpatient procedures. Clinicians use Current Procedural Terminology (CPT®) and Healthcare Common Procedure Coding System (HCPCS) Level II codes for services, procedures, and supplies, and hospitals use CPT and HCPCS Level II for outpatient procedures. Many providers focus on accurate reporting of CPT and HCPCS codes, but ICD-10-CM coding should be given equal if not more attention to ensure accuracy. While it may be the CPT/HCPCS code that determines what you get paid, it is often the ICD-10-CM code(s) that determines if you get paid.
In the oncology setting, an accurate diagnosis code assignment goes beyond assigning the correct code for the patient’s cancer. Many patients with cancer may have any number of signs, symptoms, and conditions beyond those of the neoplasm. These additional codes could be coded and reported, but for many patients, this is unlikely. Only those conditions pertinent to the primary diagnosis and part of the treatment or management by the physician of the malignant or benign disease should be coded. If a condition or symptom is a manifestation of the neoplasm, the condition or symptom is not coded or reported on the claim form. If the physician is not managing or treating the condition or symptom, the condition or symptom is not coded. Each patient’s medical record documentation will need to be reviewed per the reason for the visit or treatment to determine the appropriate codes assigned and reported.
ICD-10-CM Format
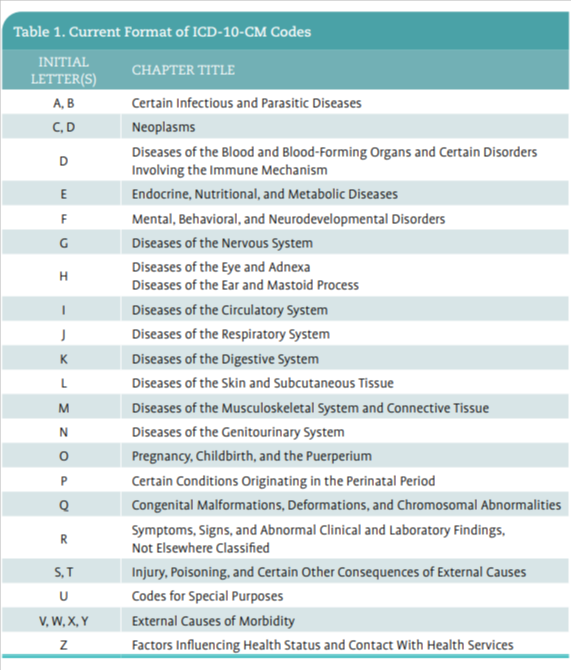
All ICD-10-CM codes begin with a letter of the alphabet and codes can be 3, 4, 5, 6, or 7 characters long. Table 1 outlines the initial letter and the corresponding disease, neoplasm, or factors influencing status that identify and assist in selecting the appropriate diagnosis code by section.
Signs and Symptoms
The ICD-10-CM guidelines indicate that the patient’s signs and symptoms can be coded even when the clinician has not confirmed a definitive diagnosis related to these signs and symptoms. Many codes for signs and symptoms are found in Chapter 18 (the R codes), but some codes are located in other chapters.
Codes are not assigned for signs and symptoms that are “associated routinely” with a disease, such as malignant neoplasms, unless the ICD-10-CM manual states otherwise. The other signs and symptoms that “may not be associated routinely with a disease process” are coded if there will be specific management or treatment of the signs and symptoms. For example, if a patient presents with dehydration following a recent drug regimen treatment, the reason for the encounter that day is to address the dehydration, not the neoplasm. The provider would report E86.0 for dehydration as the reason for the encounter as the primary code on the claim form.
Specificity
Diagnosis codes are to be used and reported at their highest number of characters available and to the highest level of specificity documented in the medical record. It is key for providers to ensure their documentation includes specificity, such as the quadrant of the breast, which third of the esophagus is involved, or the status of remission for lymphomas. The ICD-10-CM Guidelines address coding to the highest level of specificity and the need for the physician and coder to work together to ensure this occurs. “As stated in the introductory section of these official coding guidelines, a joint effort between the health care provider and the coder is essential to achieve complete and accurate documentation, code assignment, and reporting of diagnoses and procedures. The importance of consistent, complete documentation in the medical record cannot be overemphasized. Without such documentation, accurate coding cannot be achieved. The entire record should be reviewed to determine the specific reason for the encounter and the conditions treated.”2

Reason for Encounter
The guidelines indicate that the first code listed represents the “diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for the services provided.” As stated above, this may be a symptom code if the patient does not yet have an established diagnosis.
The guidelines for coding clinician services and outpatient hospital services prohibit the coding of unconfirmed conditions. This includes conditions that are described as “probable”, “suspected”, “questionable”, “rule out”, “working diagnosis”, or other similar terms. When the diagnosis is unconfirmed, the patient’s condition is coded “to the highest degree of certainty for that encounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit.”
Encounter for Therapeutic Services
Section IV of the ICD-10-CM Guidelines indicate that when the patient receives therapeutic services only, providers should code first the condition that is chiefly responsible for the services provided. However, there is an exception when the purpose of the encounter is chemotherapy or radiation therapy. Section I.C.2.e of the ICD-10-CM guidelines states:2
“If a patient admission/encounter is solely for the administration of chemotherapy, immunotherapy, or external beam radiation therapy assign code Z51.0, Encounter for antineoplastic radiation therapy, or Z51.11, Encounter for antineoplastic chemotherapy, or Z51.12, Encounter for antineoplastic immunotherapy as the first-listed or principal diagnosis. If a patient receives more than one of these therapies during the same admission, more than one of these codes may be assigned, in any sequence.
The malignancy for which the therapy is being administered should be assigned as a secondary diagnosis.
If a patient admission/encounter is for the insertion or implantation of radioactive elements (e.g., brachytherapy) the appropriate code for the malignancy is sequenced as the principal or first-listed diagnosis. Code Z51.0 should not be assigned.”
Select the code based on the type of therapy the patient will receive. If the patient receives more than 1 type of treatment during an encounter, more than 1 of these codes can be assigned, in any sequence. Secondary diagnosis codes are assigned for the cancer and for any complications that are addressed as a result of the encounter from radiation or chemotherapy.
In the case of patients receiving radiation therapy, code Z51.0 (Encounter for antineoplastic radiation therapy) is to be reported for all treatment-related services from the first day of treatment through the last day, including not only treatment delivery but also simulation, treatment devices, dosimetry planning, and physics services. Code Z51.0 is not applied to the evaluation and management (E/M) visit by the physician, as this is not considered an encounter for radiation therapy.
The ICD-10-CM guidelines state, “If a patient admission/encounter is for the insertion or implantation of radioactive elements (e.g., brachytherapy) the appropriate code for the malignancy is sequenced as the principal or first-listed diagnosis.”2 In this situation, code Z51.0 is not assigned.
If the purpose of the admission or encounter is surgical treatment and the patient also receives chemotherapy, the cancer is coded as the primary diagnosis (ICD-10-CM guidelines, Section I.C.2.e.1.). In this situation, do not assign Z51.0, Z51.11, or Z51.12. Similarly, the guidelines indicate if the reason for the encounter is to determine the extent of the cancer or to perform a procedure, such as paracentesis or thoracentesis, the diagnosis listed first is the patient’s primary or secondary cancer site, even if the patient also receives chemotherapy during the encounter.
New for 2025: Estrogen and Other Hormones and Factor Receptor Status
Approximately 2 out of 3 breast cancer diagnoses test positive for hormone receptors. Patients could have estrogen, progesterone, or both receptors telling the cancer cells to grow. Breast cancer is receptor-positive if either hormone or both are present and negative if neither are present.
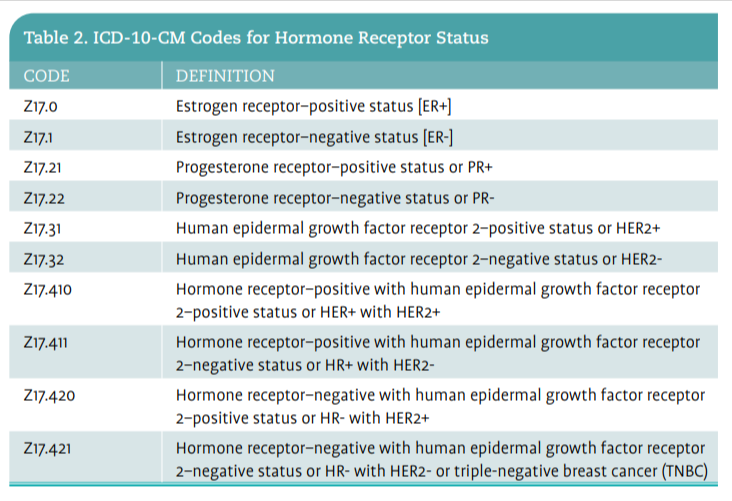
Prior to 2025, providers were directed to only “Use Additional” codes for estrogen receptor (ER) status, positive or negative. Due to revisions, providers now need to identify estrogen, progesterone, or other hormones and factor receptor status represented by codes Z17 to Z17.421.3 Understanding the receptor status of the patient is important for physicians to determine the best course of treatment.
Table 2 lists the ICD-10-CM codes for hormone receptor status; only use 1 code, as available for each receptor. Only use the code from subcategory Z17.4- when only a combined status is documented (Z17.4-Z17.421). Below is an example using the new receptor status codes:

Coding Resources for ICD-10-CM
The Centers for Disease Control and Prevention (CDC) has a website through which providers can type search words and find all of the associated neoplasm codes, drugs, external causes, and the disease index pertaining to the search. The neoplasm information lists the ICD-10-CM code by primary, secondary, carcinoma in situ, benign, uncertain behavior, and unspecified behavior for each type and location of breast cancer.
In addition, the Centers for Medicare & Medicaid Services (CMS) offers web-based training resources for both ICD-10-CM and ICD-10-PCS on its website.
Finally, Revenue Cycle Coding Strategies offers a job aid for oncology, 2025 ICD-10-CM Oncology Resource, which provides the ICD-10-CM codes associated with various anatomical sites, neoplasms, and malignancies. It can be purchased online.
Teri Bedard, BA, RT(R)(T), CPC, is executive director of client and corporate resources at Revenue Cycle Coding Strategies in Des Moines, Iowa.
References
1. World Health Organization. International statistical classification of diseases and related health problems (ICD). Accessed March 13, 2025. https://www.who.int/ standards/classifications/classification-of-diseases
2. The Centers for Disease Control and Prevention (CDC). Classification of diseases, functioning, and disability. Accessed March 1`3, 2025. https://www. cdc.gov/nchs/icd/icd-10-cm/index.html
3. The Centers for Medicare and Medicaid Services. ICD-10: what’s new. Accessed March 13, 2025. https:// www.cms.gov/medicare/coding-billing/ icd-10-codes?redirect=/ICD10












")




















